
This guide provides step-by-step instructions on completing the WC-100 Form accurately and efficiently to ensure compliance with Michigan's workers' compensation laws.
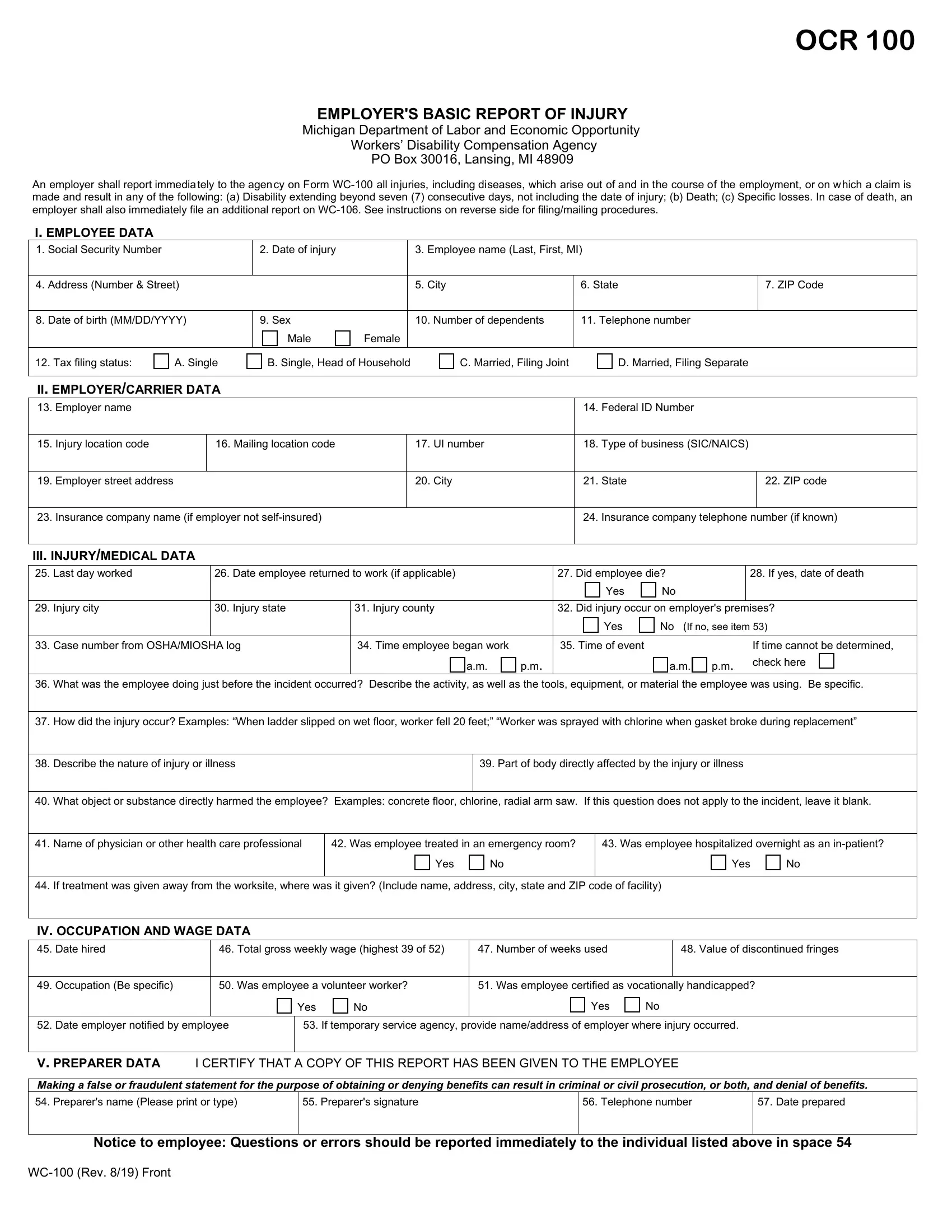
1. Employee Information
In fields 1 through 3, start by writing the employee's social security number, date of injury, and full name.
2. Additional Employee Details
Complete the employee's address, city, state, ZIP code, date of birth, gender, number of dependents, and telephone number.
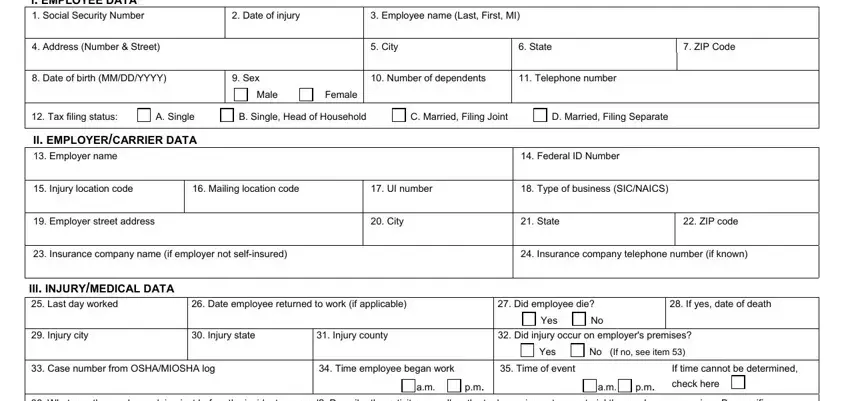
3. Tax Filing Status and Employer Details
Select the appropriate tax filing status for the employee, such as single, married, filing jointly, etc. Then, provide the employer's name and federal ID number.
4. Location and Insurance Information
Enter details about the injury location code, mailing location code, UI number, type of business (using SIC or NAICS codes), and employer's contact information. If applicable, include the insurance company name and phone number.
5. Injury and Medical Data
Record the last day worked by the employee, the date they returned to work (if applicable), and whether the employee died due to the injury. If yes, include the date of death.
6. Specific Injury Details
Describe what the employee did just before the incident, how the injury occurred, the nature of the injury or illness, the body part affected, and what directly harmed the employee.
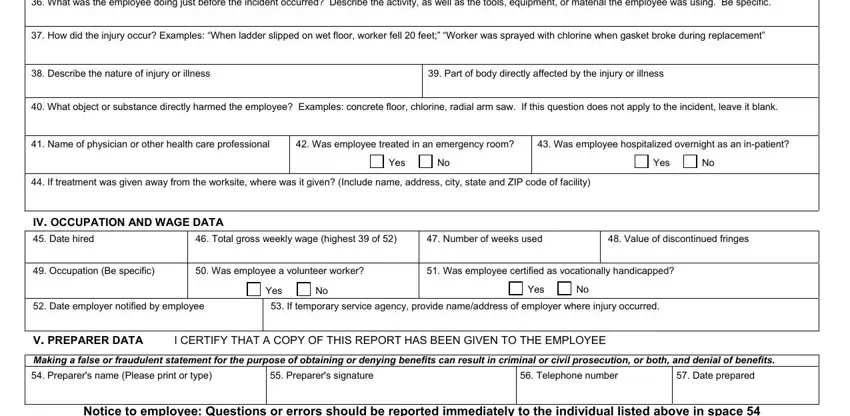
7. Medical Treatment Information
Note the name of the physician or healthcare professional who treated the employee, whether the employee was treated in an emergency room, and if they were hospitalized overnight.
8. Final Details and Submission
Complete the form by including information about the employee's occupation, wage data, and relevant information, such as whether the employee is a volunteer or certified as vocationally handicapped. Ensure that the preparer of the form provides their name, signature, and the date prepared.