
You could complete Minnesota Form R 20 easily using our PDF editor online. Our development team is ceaselessly working to improve the editor and help it become much faster for people with its multiple functions. Capitalize on present-day innovative possibilities, and discover a heap of emerging experiences! All it takes is a few easy steps:
Step 1: Access the form in our tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: After you start the online editor, you'll notice the document prepared to be completed. Other than filling in various blank fields, you could also do other sorts of things with the file, including adding custom text, editing the initial textual content, inserting images, signing the PDF, and a lot more.
When it comes to blanks of this particular document, here's what you need to know:
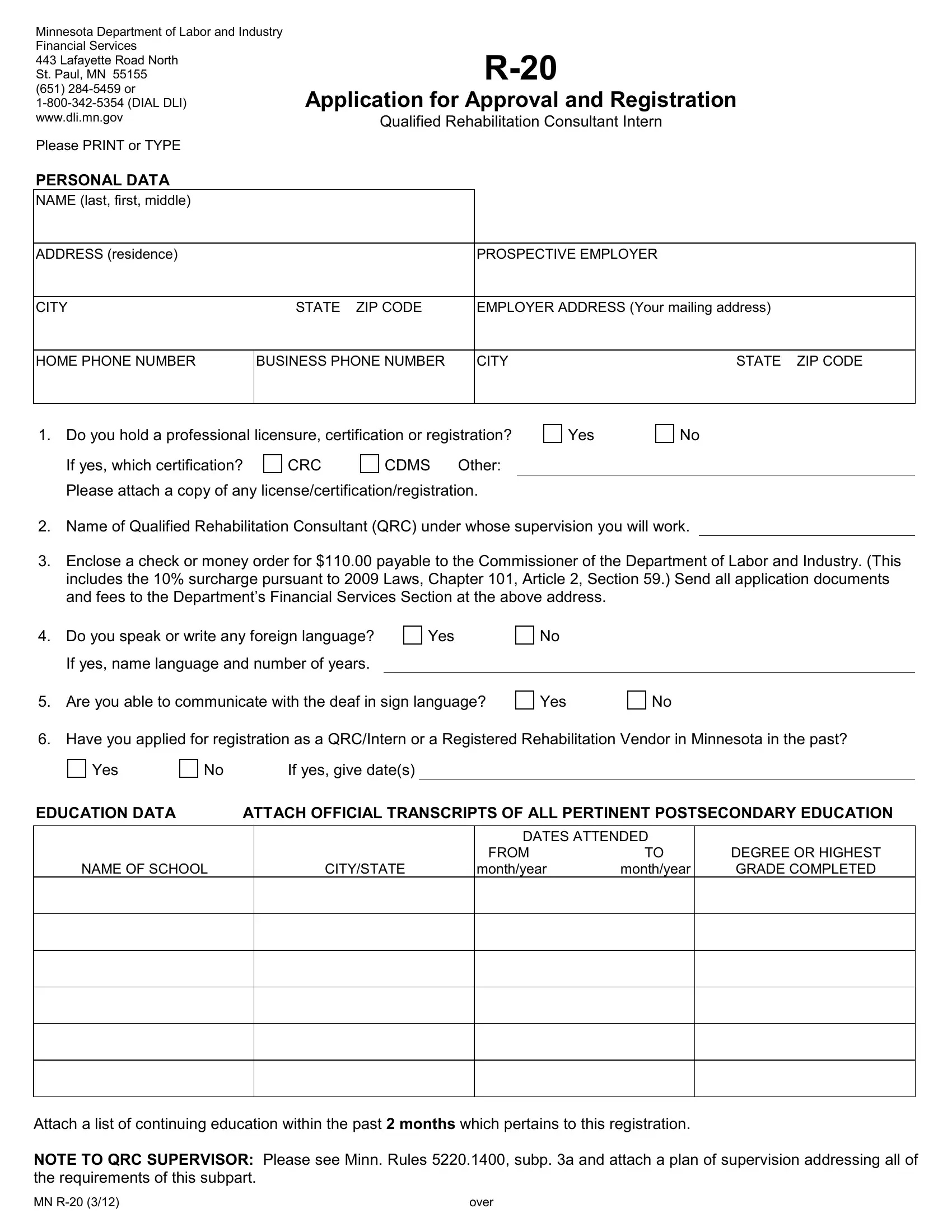
1. The Minnesota Form R 20 needs certain details to be typed in. Be sure that the following blanks are finalized:
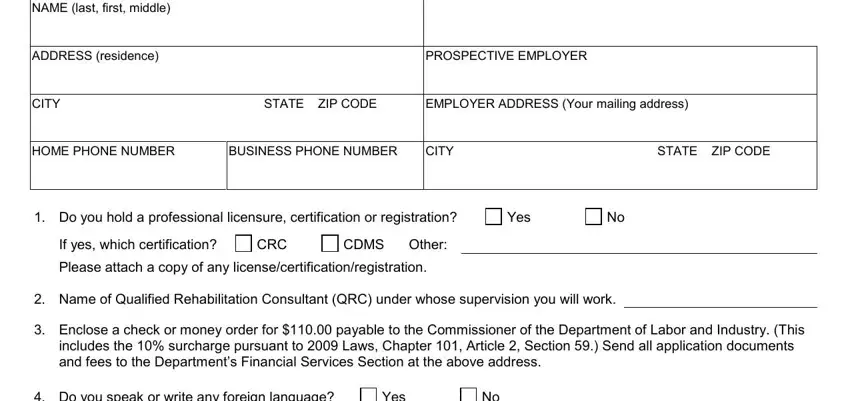
2. Your next step is usually to complete the next few blank fields: Do you speak or write any foreign, Yes, Are you able to communicate with, Yes, Have you applied for registration, If yes give dates, Yes, EDUCATION DATA, ATTACH OFFICIAL TRANSCRIPTS OF ALL, NAME OF SCHOOL, CITYSTATE, DATES ATTENDED, FROM monthyear, monthyear, and DEGREE OR HIGHEST GRADE COMPLETED.
3. This next section is focused on Attach a list of continuing, and over - fill in all of these empty form fields.

You can easily make a mistake while completing the Attach a list of continuing, and so you'll want to look again prior to when you finalize the form.
4. Filling out EMPLOYMENT HISTORY Describe in, PHONE NUMBER, ADDRESS, DATES from and to, CITY, STATE ZIP CODE, JOB TITLE, Duties, EMPLOYER NAME, ADDRESS, PHONE NUMBER, IMMEDIATE SUPERVISOR NAME, DATES from and to, CITY, and STATE ZIP CODE is key in this fourth step - don't forget to be patient and take a close look at every blank!
Step 3: Spell-check what you have entered into the form fields and hit the "Done" button. Sign up with FormsPal today and immediately gain access to Minnesota Form R 20, set for download. All changes made by you are saved , allowing you to customize the form at a later point if necessary. At FormsPal, we aim to guarantee that all of your details are stored secure.