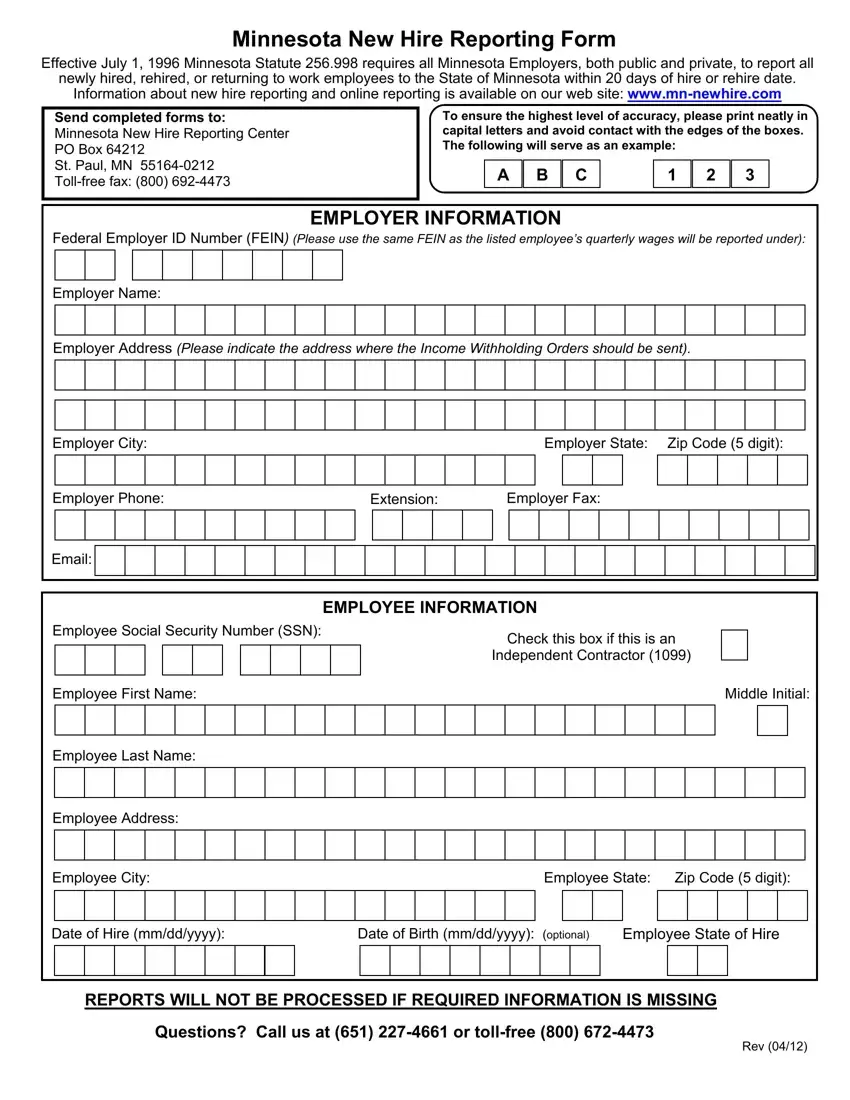
The Minnesota New Hire Reporting form plays a critical role in enforcing child support obligations and ensuring the accuracy of unemployment and workers' compensation benefits. Incepted on July 1, 1996, under Minnesota Statute 256.998, this mandate calls for all employers, spanning both the public and private sectors, to report new hires, rehires, or employees returning to work within a stipulated 20-day period. This process, while geared towards maintaining the integrity of various state benefits, also aids in the detection and prevention of fraud. Employers are directed to send completed forms to the Minnesota New Hire Reporting Center, with detailed instructions provided for the accurate and neat input of information to avoid processing delays. Both employee and employer information is crucial, with specific emphasis on the Federal Employer ID Number (FEIN) associated with quarterly wage reports, and accurate employee details including social security numbers, names, and addresses. The option to report online enhances the convenience and efficiency of this critical reporting requirement. Inquiries and concerns are handled through designated toll-free numbers, ensuring support is readily available for employers navigating the reporting process.
| Question | Answer |
|---|---|
| Form Name | Minnesota New Hire Reporting Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mn new hire reporting, minnesota new hire, mn hire form, mn new hire form |
