


mn universal credentialing application can be completed online in no time. Just open FormsPal PDF editor to perform the job right away. FormsPal team is devoted to making sure you have the perfect experience with our editor by consistently adding new features and improvements. With all of these updates, working with our tool becomes better than ever! Here's what you'll need to do to get started:
Step 1: First, open the tool by pressing the "Get Form Button" above on this page.
Step 2: Using our advanced PDF tool, you are able to do more than just fill in blank form fields. Edit away and make your forms look great with customized text incorporated, or modify the file's original content to perfection - all comes with the capability to incorporate your personal graphics and sign it off.
As a way to fill out this form, be certain to type in the right details in each blank field:
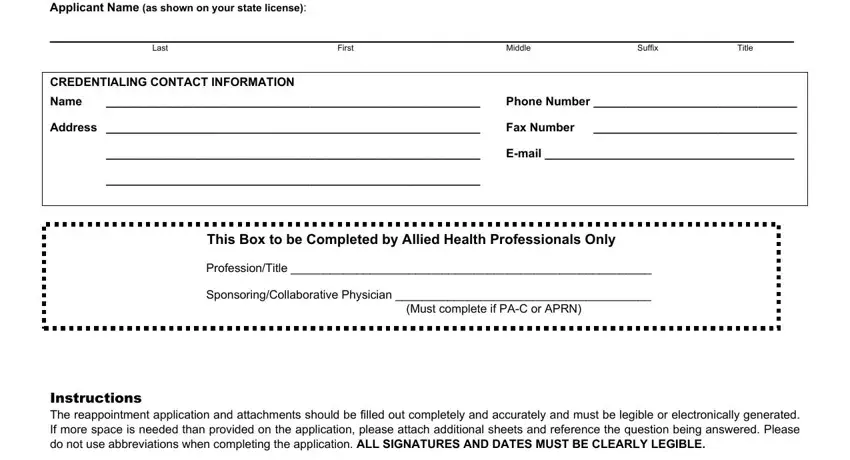
1. Before anything else, when filling in the mn universal credentialing application, start in the part that includes the next fields:
2. When this part is done, you have to include the required specifics in Provided complete street address, employment hospital affiliations, Designate dates by month day and, Answered all of the Disclosure, Signed and dated the Attestation, Signed and dated the, and All Information Must Be Printed in in order to proceed further.
You can certainly get it wrong when filling out your Signed and dated the Attestation, consequently make sure that you go through it again before you decide to finalize the form.
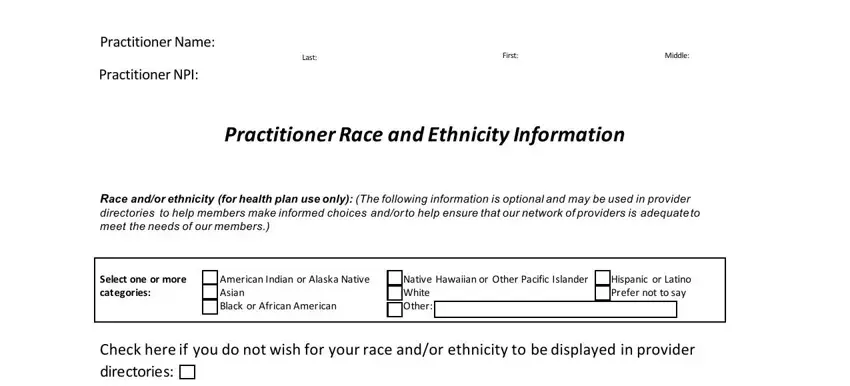
3. This next section is mostly about Practitioner Name, Practitioner NPI, Last, First, Middle, Practitioner Race and Ethnicity, Race andor ethnicity for health, Select one or more categories, American Indian or Alaska Native, Native Hawaiian or Other Pacific, Hispanic or Latino Prefer not to, and Check here if you do not wish for - fill out each one of these blanks.
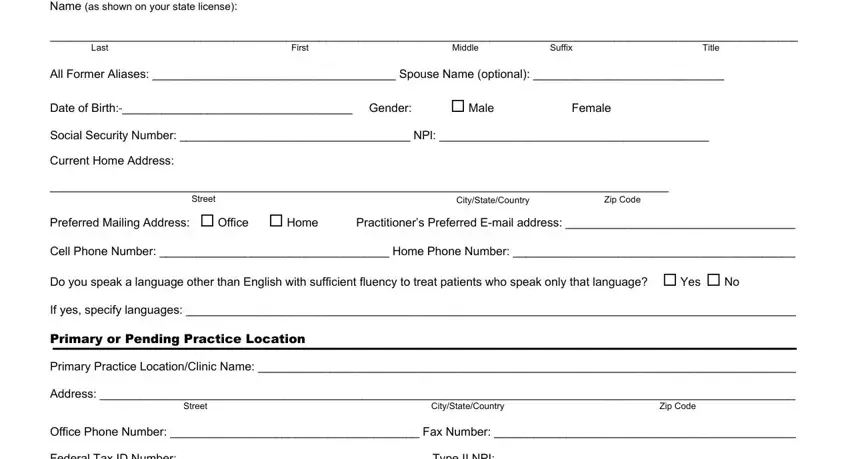
4. It's time to complete this fourth part! Here you'll get these Name as shown on your state license, Last, First, Middle, Suffix, Title, All Former Aliases Spouse Name, Date of Birth Gender, Male Female, Social Security Number NPl, Current Home Address, Street, CityStateCountry, Zip Code, and Preferred Mailing Address Office fields to fill out.
5. And finally, the following last portion is what you'll want to wrap up prior to closing the PDF. The blank fields at this stage are the following: Federal Tax ID Number Type II NPI, Email Address, Start Date at this location, Practicing as Primary Care, Hospital Based only, Other specify, Accepting new patients Yes No, Directory Suppress Yes No, Primary Specialty in which care, Sub Specialty ies in which care, and Provide a narrative description of.
Step 3: Make sure your details are correct and just click "Done" to conclude the task. Get your mn universal credentialing application after you sign up for a free trial. Easily view the pdf form in your personal cabinet, with any edits and changes being all kept! FormsPal ensures your information privacy via a secure system that in no way records or shares any type of private data involved in the process. You can relax knowing your docs are kept confidential any time you work with our tools!