|
Medical Marijuana Registry |
|
|
AP |
|
4300 Cherry Creek Drive South, Denver, CO 80246-1530 303-692-2184 |
|
|
|
E-mail: medical.marijuana@state.co.us Website: www.cdphe.state.co.us/hs/medicalmarijuana |
|
|
|
|
|
|
|
|
|
Application Instructions
Colorado Medical Marijuana registration cards are available only for Colorado residents being treated for an active, chronic or debilitating medical condition. To apply for a registration card, please complete an application packet as described below. If you make a mistake, please complete a new form. Do not write over, white-out or cross-out information. This will void the form.
A complete application packet includes:
1.An application for registration card completed by you, signed and notarized.
2.A physician certification completed by your doctor.
3.A copy of your Colorado ID. If you do not have a Colorado ID, submit proof of identity and Colorado residency.
4.A copy of your caregiver’s valid ID and form #MMR1012 Caregiver Acknowledgement, if a caregiver is selected.
5.A form of payment or a Request for Fee Waiver/Tax Exempt Status form and supporting materials.
1.Medical Marijuana Registry Application
a.Please complete the entire application. Write or type clearly and neatly.
b.Patient social security number: Social security numbers are required for application submission. The Registry uses a patient’s social security number as a unique number for tracking records. Article XVIII, 14(3)(b)(II) of the Colorado Constitution states: “In order to be placed on the state’s confidential registry for the medical use of marijuana, a patient must … submit the completed application form adopted by the state health agency, including the following information … (II) The name, address, date of birth, and social security number of the patient …” VISA/ITIN numbers are not accepted as a replacement for social security numbers.
c.Mark your application as ‘NEW’ if you have never had a card with the Registry. If you have had a card, regardless of the year, mark your application as ‘RENEWAL.’
d.Submit renewal applications between 45 to 60 days before your card expires to allow time for processing. Renewal applications more than 60 days before the card expiration date are rejected as duplicate applications. Any fees sent with a duplicate application are non-refundable and are not credited toward future applications.
e.Ensure the mailing address is complete, including apartment or lot number. Mail returned to the Registry by the post office is retained for 90 days then shredded.
f.You may select to have a caregiver or a medical marijuana center. It is not required to have either. The provider will not be printed on your card, if provider information is incomplete or caregiver ID is not included.
g.If you list a caregiver, you must also submit form #MMR1012 Caregiver Acknowledgement and a copy of the caregiver’s ID with your application.
h.If you are under the age of 18 or homebound, you may choose both a caregiver and a medical marijuana center.
i.Sign and date this form in front of a notary. The date of your signature and the notary’s signature must be the same.
j.The form cannot be notarized by the patient, the caregiver, the physician or the person who signs the payment.
2.Physician Certification
a.Your physician must complete, sign, and date the physician certification.
b.The signing physician must be an MD or DO with an active Colorado medical license. Physicians with conditions or restrictions on their licenses, or out-of-state licenses, are not accepted.
c.The Registry must receive your complete, correct application packet within 60 days of the physician’s signature. Application packets with physician certifications more than 60 days old are rejected.
d.The Registry cannot accept paperwork on security paper that reads “VOID” when copied.
3.Proof of Identity and Residency (see page 2 for Proof of Identity and Colorado Residency requirements) – Please do not send the original document. Send a clear, readable and complete copy.
a.Medical Marijuana Registration cards are available only to Colorado residents. You must provide proof of your identity and residency. Damaged, expired or tampered IDs are not valid.
b.The name on your application must match the name on your ID. If you have had a change of name since you last submitted paperwork to the Registry, provide a copy of the certified document proving name change (such as marriage license, divorce decree, or legal name change documents).
c.To ensure your ID is readable, please enlarge it on a copier at 150% to 200% and lighten background slightly.
4.Authorized Representatives – If patient care rights and responsibilities have been legally assigned to
another person, a copy of the legal documentation must be submitted with the application. Acceptable documents include court-certified guardianship documents, power of attorney or medical power of attorney. Medical care rights must be included as a responsibility of the guardian/agent in order to contact the Registry regarding patients' records and care. A copy of the care provider’s ID is also required.
5.Application packets must be sent separately. Only one application packet and check/money order per envelope. If sending by certified mail, certify each envelope separately.
MMR1001 – Adult Application – Revised January 2014 |
Page 1 of 8 |
Application Instructions
6.Please allow 4 to 6 weeks from the date the Registry receives your paperwork for application processing. If you have not received a response within 6 weeks, please contact the Registry at 303-692-2184, ext. 3. Your paperwork or card will be mailed to the address on your application. The Registry does not mail cards outside of the state.
7.DO NOT send in any additional paperwork to support your application, unless requested by the Registry. Any non-required paperwork is shredded.
PROOF OF IDENTITY AND COLORADO RESIDENCY
Please do not send original documents. Send a clear, readable copy.
One (1) of the following: |
Two (2) of the following: |
• |
Colorado driver’s license |
Minimum of one (1) ID from the group below - |
• |
Colorado ID |
• |
Out-of-state driver’s license or ID |
• |
Temporary Colorado driver’s license OR |
• |
U.S. Passport or Passport Card |
• |
Temporary Colorado ID |
• |
U.S. Military ID (copy of front and back) |
|
|
• |
Tribal ID |
Proof of residency is not required if |
And a minimum of one (1) proof of residency from the group below - |
• |
Proof of Colorado employment (paycheck stub/W-2/certified Colorado tax return) |
submitting a Colorado-issued ID. |
• |
Copy of an entire government-issued benefit letter (PERA, SSI, Disability, etc.) |
|
|
• |
Copy of a Colorado-issued certification (such as nursing, electrician, etc.) |
|
|
• |
Copy of a utility bill. All addresses on the bill must be in Colorado. |
If you do not have the above documents, please contact the Registry at 303-692-2184 (ext. 3) to discuss other options.
i.All documents must be currently valid when received at the Registry.
ii.Damaged, expired, or tampered IDs are not valid.
iii.The address on the ID does not have to match the mailing address on the application.
iv.All IDs must be verifiable and have specific issue and expiration dates.
v.At least one document must show the patient’s date of birth.
vi.Passports must include full photo page and the signed signature page. Passport cards must include copy of front and back.
vii.Proof of residency materials must be dated within 60 days of the date the Registry receives them, unless otherwise noted.
viii.As proof of Colorado employment, the W-2 or certified Colorado tax return must be for the most recent tax year and have a Colorado mailing address.
ix.Bills from telephone, electricity, water, trash, cable, or internet providers are considered valid and verifiable utility bills. Bills must include the organization name, logo and contact information.
x.All government benefit letters must include the issuing agency’s logo and contact information; the patient’s name and address; and an account or case number. Examples of acceptable benefit letters include PERA, Medicaid/Medicare, Food Stamps/Food Assistance, TANF, and Social Security.
xi.Certification documents must include the patient’s Colorado address, be issued by a Colorado state agency and be dated within the last year.
8.Non-refundable $15 application fee or Request for Fee Waiver/Tax Exempt Status form:
The following application fee and fee waiver processes are effective for applications received February 1, 2014 or later.
a.To pay $15 application fee: Make check or money order payable to CDPHE. We do not accept temporary checks. Do not send cash. Please write the patient’s name on the payment. Make sure the form of payment is signed. The notary cannot sign the form of payment. The date of payment must be less than one (1) year old when received at the Registry. All monies received by the Registry are nonrefundable.
b.To request a fee waiver: You must submit a Request for Fee Waiver/Tax Exempt Status form (#MMR1010) and a certified copy of a current Colorado tax return with your application packet. You may qualify for a fee waiver if your household income is at 185% of the Federal Poverty Level or less. The chart below indicates the annual household incomes, adjusted for family size, that qualify for a fee waiver.
Household incomes at 185% of 2013 Federal Poverty Guidelines*
Source: Federal Register, Vol. 78, No. 16, January 24, 2013, pp. 5182-5183.
# in Family |
|
Annual Income |
1 |
$ |
21,257 |
2 |
$ |
28,694 |
3 |
$ |
36,130 |
|
|
|
4 |
$ |
43,567 |
|
|
|
5 |
$ |
51,005 |
|
|
|
6 |
$ |
58,442 |
|
|
|
7 |
$ |
65,879 |
8 |
$ |
73,316 |
Each additional |
$ |
7,437 |
*Poverty guidelines are updated periodically in the Federal Register by the U.S. Department of Health and Human Services under the authority of 42 U.S.C. 9902(2)
MMR1001 – Adult Application – Revised January 2014 |
Page 2 of 8 |
Application Instructions
9.Submit all items by mail or deliver to the Registry’s drop-box. The Registry does not accept forms by fax or e-mail.
Mail To: |
Drop-Box: |
|
Colorado Dept. of Public Health & Environment |
Application Processing |
710 S. Ash Street, Southeast Entrance |
CDPHE |
Open: Monday-Friday, 7:00 a.m. to 6:00 p.m. |
HSV-8608 |
The drop box is on the wall inside the first set of glass doors. Your paperwork |
4300 Cherry Creek Drive South |
must be in a sealed envelope. You will not receive a receipt. If you wish to have |
Denver, CO 80246-1530 |
a receipt, please mail in your paperwork by certified mail. |
Application Packet Checklist:
The application is complete and accurate.
The application was signed and dated by you and a notary.
The dates of your signature and the notary’s signature match.
The physician certification is complete and accurate.
The date of the physician’s signature is current. Mail your application packet as soon as possible after your physician signs the physician certification.
There are no areas on any of the forms where information has been written over, crossed out or white-out was used.
You have included a clear copy of your valid Colorado ID.
If you do not have a Colorado ID, you have included a clear copy of your ID and proof of residency.
If included, all copies of utility or cable bills show the mailing address, not just a service address. All addresses must be in Colorado.
You have made copies of all the documents you are sending to the Registry.
You have included a form of payment or the Request for Fee Waiver/Tax-Exempt Status form, including a certified copy of your Colorado tax return.
Submit your application packet for yourself. Do not allow anyone else to submit the paperwork for you.
Send your application packet by certified mail to have proof of submission. Keep the mail receipt.
Questions can be sent by e-mail to medical.marijuana@state.co.us or by phone at 303-692-2184 (ext. 3). Application Review Process:
1.Initial Review: The Registry reviews all applications against criteria described in the application Instructions. The nonrefundable application fee, if included in the application packet, is deposited.
2.Approved Application: If an application packet is complete and has all supporting materials, a card is mailed.
3.Rejected Application: If an application packet is inaccurate or incomplete, the Registry processes the payment and keeps the submitted paperwork. A rejection letter detailing corrections needed is sent to the patient. With each rejection, patients are given 60 days to make corrections without paying additional application fees. Patients are given two (2) opportunities to submit corrections to the Registry.
4.Approved Corrections: When corrections are submitted to the Registry, they are reviewed for accuracy and completeness. If the application packet is complete after corrections, a card is mailed to the patient.
5.Corrections Beyond 60-Days: Patients who do not submit corrections within the 60-day window must submit a new application packet including a new physician certification and an additional $15 application fee.
6.Denial: The application is denied after the patient has submitted inaccurate or incomplete paperwork three times (the original application plus two correction attempts). The patient will have to wait six (6) months before re-applying for a Medical Marijuana Registration card, if the application is denied.
7.Appeals: If an application is denied, or the Registry suspends or revokes the patient’s current registration card, a notice will be sent to the patient with details regarding the reason for denial, suspension or revocation. If the patient disagrees with a final decision from the Registry, the patient may send a letter to the Registry requesting an appeals hearing. The request for a hearing must be received by the Registry within thirty (30) calendar days from the date of the postmark on the notice.
For more information, please visit www.cdphe.state.co.us/hs/medicalmarijuana or call 303-692-2184.
The Registry is not affiliated with any privately operated club, organization, or dispensary.
MMR1001 – Adult Application – Revised January 2014 |
Page 3 of 8 |
|
|
|
|
|
|
|
|
|
|
Medical Marijuana Registry |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AP |
|
|
|
|
|
|
|
|
|
|
|
4300 Cherry Creek Drive South, Denver, CO 80246-1530 303-692-2184 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E-mail: medical.marijuana@state.co.us Website: www.cdphe.state.co.us/hs/medicalmarijuana |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STAFF |
|
|
Application for Registration Card |
|
|
|
|
|
ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carefully complete the packet. Do not make corrections to the form. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
See instructions on page 1. Proof of identity required with all forms. |
|
|
|
|
|
|
|
|
|
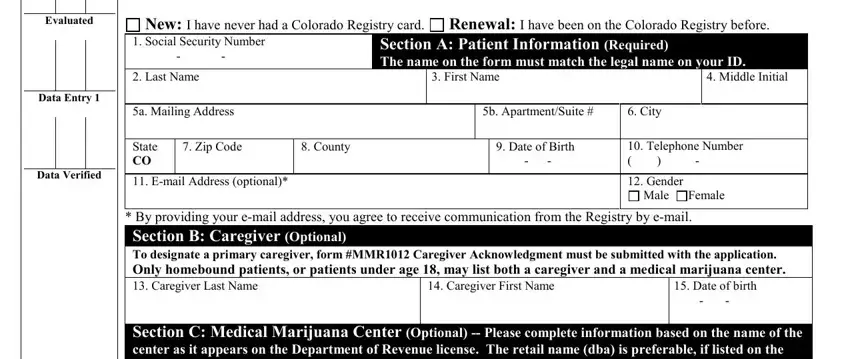
New: I have never had a Colorado Registry card. Renewal: I have been on the Colorado Registry before. |
|
|
|
Evaluated |
|
|
|
|
|
|
|
|
|
|
1. Social Security Number |
|
|
|
Section A: Patient Information (Required) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The name on the form must match the legal name on your ID. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last Name |
|
|
|
|
3. First Name |
|
|
4. Middle Initial |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Data Entry 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5a. Mailing Address |
|
|
|
|
|
5b. Apartment/Suite # |
6. City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
|
7. Zip Code |
|
8. County |
|
|
|
|
9. Date of Birth |
10. Telephone Number |
|
|
|
|
|
|
|
|
CO |
|
|
|
|
|
- - |
( ) |
- |
|
|
|
|
Data |
Verified |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. E-mail Address (optional)* |
|
|
|
|
|
12. Gender |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
Female |
|
*By providing your e-mail address, you agree to receive communication from the Registry by e-mail.
Section B: Caregiver (Optional)
To designate a primary caregiver, form #MMR1012 Caregiver Acknowledgment must be submitted with the application.
Only homebound patients, or patients under age 18, may list both a caregiver and a medical marijuana center.
13. Caregiver Last Name |
14. Caregiver First Name |
15. Date of birth |
|
|
- - |
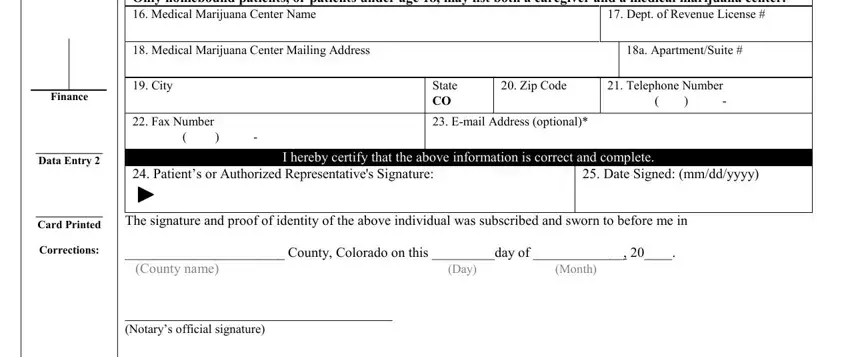
Section C: Medical Marijuana Center (Optional) -- Please complete information based on the name of the center as it appears on the Department of Revenue license. The retail name (dba) is preferable, if listed on the license.
Only homebound patients, or patients under age 18, may list both a caregiver and a medical marijuana center.
|
|
|
16. |
Medical Marijuana Center Name |
|
|
|
17. Dept. of Revenue License # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. |
Medical Marijuana Center Mailing Address |
|
|
|
|
18a. Apartment/Suite # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. City |
|
|
State |
20. Zip Code |
21. Telephone Number |
Finance |
|
|
|
|
|
CO |
|
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22. |
Fax Number |
|
|
23. E-mail |
Address (optional)* |
|
|
|
|
____________ |
|
|
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Data Entry 2 |
|
|
|
|
I hereby certify that the above information is correct and complete. |
|
|
____________ |
|
|
24. Patient’s or Authorized Representative's Signature: |
|
25. Date Signed: (mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
The signature and proof of identity of the above individual was subscribed and sworn to before me in |
|
Card Printed |
|
Corrections: |
_______________________ County, Colorado on this _________day of _____________, 20____. |
|
|
|
|
|
|
(County name) |
|
(Day) |
(Month) |
|
|
|
|
___________________________________ |
|
(Notary’s official signature) |
|
___________________________________ |
|
(Commission expiration date) |
AFFIX NOTARY SEAL |
MMR1001 – Adult Application – Revised January 2014 |
Page 4 of 8 |
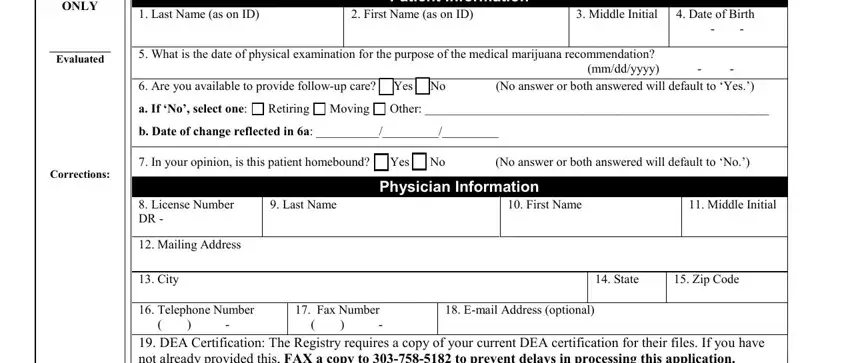
Physician Certification Instructions
1.Complete the entire form, sign and date.
2.If you make a mistake on this form, please complete a new form. Do not write over, white-out or cross-out information. This will void the form.
3.Patients must have a new physical exam each year as part of their renewal process. Ensure the exam date reflects the most current patient information.
4.Please keep a copy of the form in the patient’s medical record. To avoid fraud, the Registry verifies all physician signatures. You will receive a verification letter for patients in the months the Registry receives physician certifications with your signature.
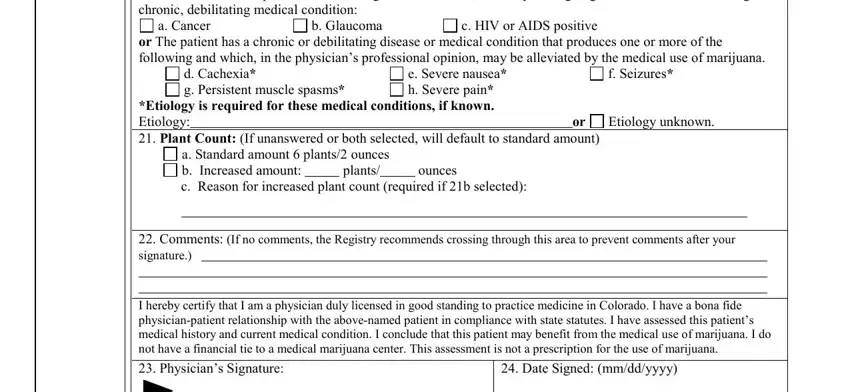
5.Auto defaults:
OIf question #7 is incomplete or both boxes are selected, the auto-default response is “no.”
OIf question #21 is incomplete, the auto-default response is “standard amount.”
6.Please do not fax or e-mail the form to the Registry. The patient must submit the physician certification along with his or her complete Medical Marijuana Registry application packet.
7.This does not constitute a prescription for marijuana.
8.To sign the form, you must be an MD or DO with an active Colorado medical license. Physicians with conditions or restrictions on their licenses, or out-of-state licenses, are not accepted.
9.A copy of your current DEA certification must be on file with the Registry. If you have not already provided this, please fax a copy to 303-758-5182. If your DEA is not on file when we receive your patient’s paperwork, it will be rejected.
10.The Registry cannot accept paperwork on security paper that reads “VOID” when copied.
11.Encourage patients to submit their application packets as soon as possible after you sign the physician certification. The Registry rejects physician certifications that are more than 60 days old.
12.The Registry has included in the application packet, for your review, “Regulation 8: Physician requirements; reasonable cause for referrals of physicians to the Colorado Medical Board; reasonable cause for department adverse action concerning physicians; appeal rights.” For a link to the complete Board of Health rules, please visit our website www.cdphe.state.co.us/hs/medicalmarijuana.
13.You may contact the Registry at medical.marijuana@state.co.us or (303) 692-2184, if you have any questions.
MMR1001 – Adult Application – Revised January 2014 |
Page 5 of 8 |