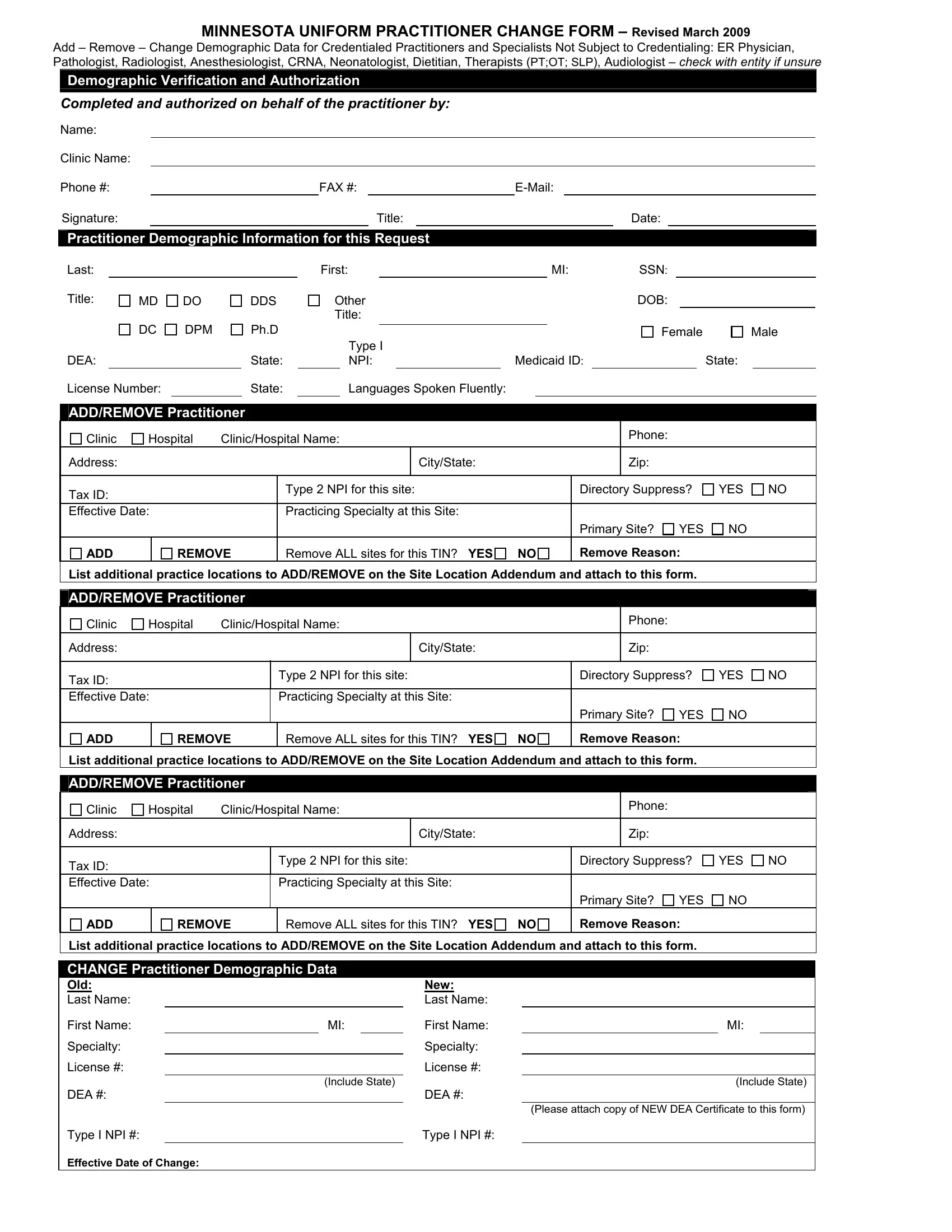
In March 2009, the Minnesota Uniform Practitioner Change Form was revised to streamline the management of practitioner information across the healthcare sector in Minnesota. This comprehensive document facilitates the addition, removal, or modification of demographic data for credential practitioners including, but not limited to, Emergency Room Physicians, Pathologists, Radiologists, Anesthesiologists, Certified Registered Nurse Anesthetists (CRNA), Neonatologists, Dietitians, Therapists (Physical, Occupational, Speech-Language), and Audiologists. It mandates specific details about the practitioner such as their name, social security number, professional titles, date of birth, gender, language fluency, practicing specialty, and essential identifiers like DEA, NPI, and Medicaid ID numbers. Clinic or hospital affiliations can also be updated through this form, requiring information on practice locations' addresses, tax identification numbers, and the effective dates for any changes. An additional Site Location Addendum Form is provided for practitioners changing associations with more than three sites, ensuring all necessary information is accurately captured and processed effectively. This documentation is crucial for maintaining accurate directories and ensuring compliance with various regulations, aiming to enhance communication within the healthcare system and between practitioners and institutions.
| Question | Answer |
|---|---|
| Form Name | Mn Uniform Change Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | minnesota practitioner change, mn uniform practitioner change form, mn uniform practitioner change form bcbs, uniform change form |
MINNESOTA UNIFORM PRACTITIONER CHANGE FORM – Revised March 2009
Add – Remove – Change Demographic Data for Credentialed Practitioners and Specialists Not Subject to Credentialing: ER Physician, Pathologist, Radiologist, Anesthesiologist, CRNA, Neonatologist, Dietitian, Therapists (PT;OT; SLP), Audiologist – check with entity if unsure
Demographic Verification and Authorization
Completed and authorized on behalf of the practitioner by:
Name:
Clinic Name:
Phone #: |
|
FAX #: |
|||||||
Signature: |
|
|
|
Title: |
|
|
|
Date: |
|
Practitioner Demographic Information for this Request
Last: |
|
|
|
First: |
|
|
|
MI: |
SSN: |
||
Title: |
MD |
DO |
DDS |
Other |
|
|
|
DOB: |
|||
|
|
|
|
Title: |
|
|
|
|
|
||
|
DC |
DPM |
Ph.D |
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
Type I |
|
|
|
|
|
|
DEA: |
|
|
State: |
|
NPI: |
|
Medicaid ID: |
|
State: |
||
Male
License Number: |
|
State: |
|
Languages Spoken Fluently: |
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
|
|
|
|
|
|
|
|
ADD |
REMOVE |
Remove ALL sites for this TIN? YES NO |
Remove Reason: |
||||
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
|
|
|
|
|
|
|
|
ADD |
REMOVE |
Remove ALL sites for this TIN? YES NO |
Remove Reason: |
||||
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
CHANGE Practitioner Demographic Data
Old: |
|
|
New: |
|
|
|
|
Last Name: |
|
|
|
Last Name: |
|
|
|
First Name: |
|
MI: |
|
First Name: |
|
MI: |
|
Specialty: |
|
|
|
Specialty: |
|
|
|
License #: |
|
|
License #: |
|
|
|
|
|
|
(Include State) |
|
|
(Include State) |
||
DEA #: |
|
|
DEA #: |
|
|
|
|
|
|
|
|
|
(Please attach copy of NEW DEA Certificate to this form) |
||
Type I NPI #: |
|
|
|
Type I NPI #: |
|
|
|
Effective Date of Change: |
|
|
|
|
|
|
|
THE FOLLOWING SITE LOCATION ADDENDUM FORM IS USED IN CONJUNCTION WITH THE MINNESOTA UNIFORM PRACTITIONER CHANGE FORM WHEN ADDING OR REMOVING PRACTITIONERS FROM MORE THAN THREE SITES. THIS FORM WILL ONLY BE ACCEPTED WHEN IT IS ACCOMPANIED BY A COMPLETED MINNESOTA UNIFORM PRACTITIONER CHANGE FORM.
SITE LOCATION ADDENDUM
Must indicate if the additional site(s) are being ADDED or REMOVED
ADDITIONAL LOCATION(s) FOR:
Last: |
|
First: |
|
MI: |
|
SSN: |
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
|
|
|
|
|
|
|
|
|
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
||||
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
Location addendum.doc – March 2009