
If you need to fill out humana change form, it's not necessary to download and install any sort of programs - simply try using our online tool. Our expert team is relentlessly working to expand the tool and make it much easier for people with its many functions. Benefit from today's progressive possibilities, and find a heap of new experiences! Starting is easy! All you have to do is stick to these simple steps directly below:
Step 1: Press the "Get Form" button above on this webpage to access our PDF tool.
Step 2: This editor provides you with the opportunity to customize your PDF document in various ways. Transform it by adding your own text, adjust what is originally in the document, and include a signature - all at your convenience!
Completing this PDF needs focus on details. Ensure that all necessary areas are completed correctly.
1. Whenever filling in the humana change form, ensure to incorporate all of the important blanks in the associated area. It will help facilitate the work, making it possible for your information to be processed fast and accurately.
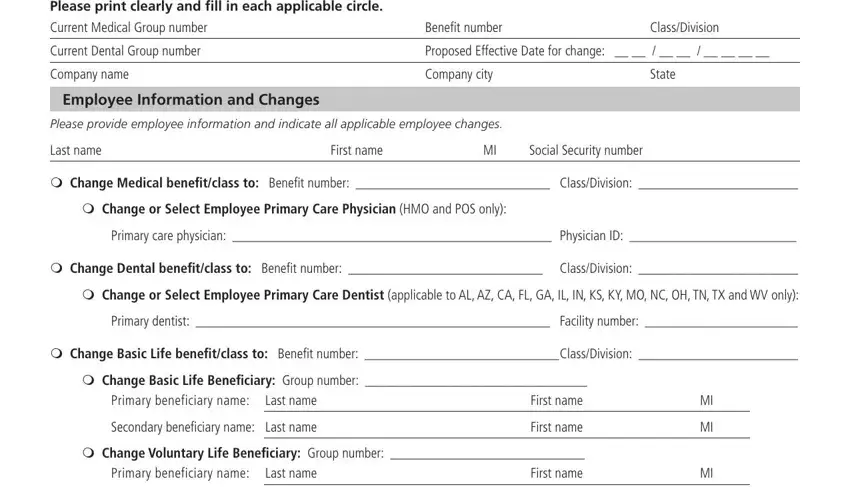
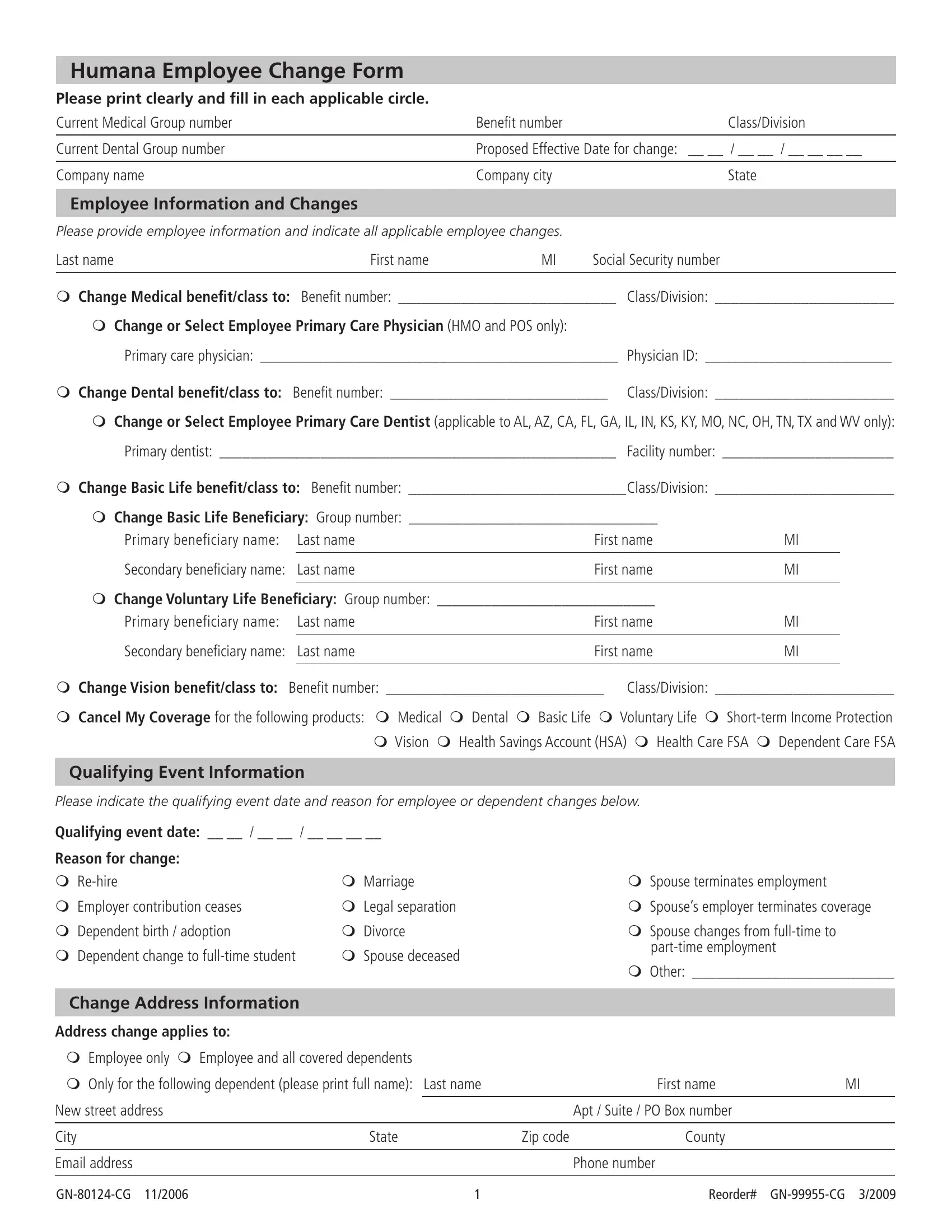
2. The third step is usually to complete these particular blank fields: Secondary beneiciary name Last name, First name, m Change Vision beneitclass to, ClassDivision, m Cancel My Coverage for the, Qualifying Event Information, Please indicate the qualifying, Qualifying event date, Reason for change m Rehire m, m Marriage m Legal separation m, Change Address Information, Address change applies to, m Employee only m Employee and all, m Only for the following dependent, and m Spouse terminates employment m.
3. The next stage is straightforward - fill in every one of the blanks in m Only for the following dependent, New street address, City, Email address, GNCG, State, First name, Apt Suite PO Box number, Zip code, County, Phone number, and Reorder GNCG in order to complete this process.

It's easy to make a mistake while completing the New street address, consequently make sure you take a second look prior to deciding to submit it.
4. This part comes with these particular blanks to type in your details in: Group Number, Social Security Number, Dependent Changes, Please complete this section for, Last name, First name, Date of birth, Social Security number Dependent, Gender m Female m Male, Relationship m Spouse m Child m, If disabled indicate reason, m Add or m Delete dependent tofrom, m Voluntary Life m Vision, m Dental m Basic Life, and Primary care physician Physician.
5. Last of all, the following final subsection is what you need to wrap up prior to closing the document. The fields here are the next: Primary care physician Physician, m Change or Select DHMO applicable, Primary dentist Facility number, Last name, First name, Date of birth, Social Security number Dependent, Gender m Female m Male, Relationship m Spouse m Child m, If disabled indicate reason, m Add or m Delete dependent tofrom, m Voluntary Life m Vision, m Dental m Basic Life, Primary care physician Physician, and m Change or Select DHMO applicable.
Step 3: Once you've glanced through the information provided, press "Done" to complete your FormsPal process. After registering afree trial account here, it will be possible to download humana change form or email it right off. The PDF file will also be at your disposal via your personal account with your every modification. When using FormsPal, it is simple to complete documents without worrying about data leaks or entries getting shared. Our protected system makes sure that your personal data is stored safe.