The Minnesota Uniform Change Form is an important document that every employer in the state of Minnesota should be familiar with. This form is designed to help employers keep track of their employees’ changing schedule needs, ensuring all requirements are met and any alterations or adjustments regarding hours or days worked are properly authorized. It's important for team members to know this form exists and understand how to properly fill it out so there is no confusion about who is entitled to what days off and when those changes need to be implemented. In this blog post, we'll discuss the use of the Minnesota Uniform Change Form and provide detailed information on its contents, filing instructions, potential problems associated with improper filing processes, as well as answer some frequently asked questions related to uniform change forms in general.
| Question | Answer |
|---|---|
| Form Name | Mn Uniform Change Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | minnesota practitioner change, mn uniform practitioner change form, mn uniform practitioner change form bcbs, uniform change form |
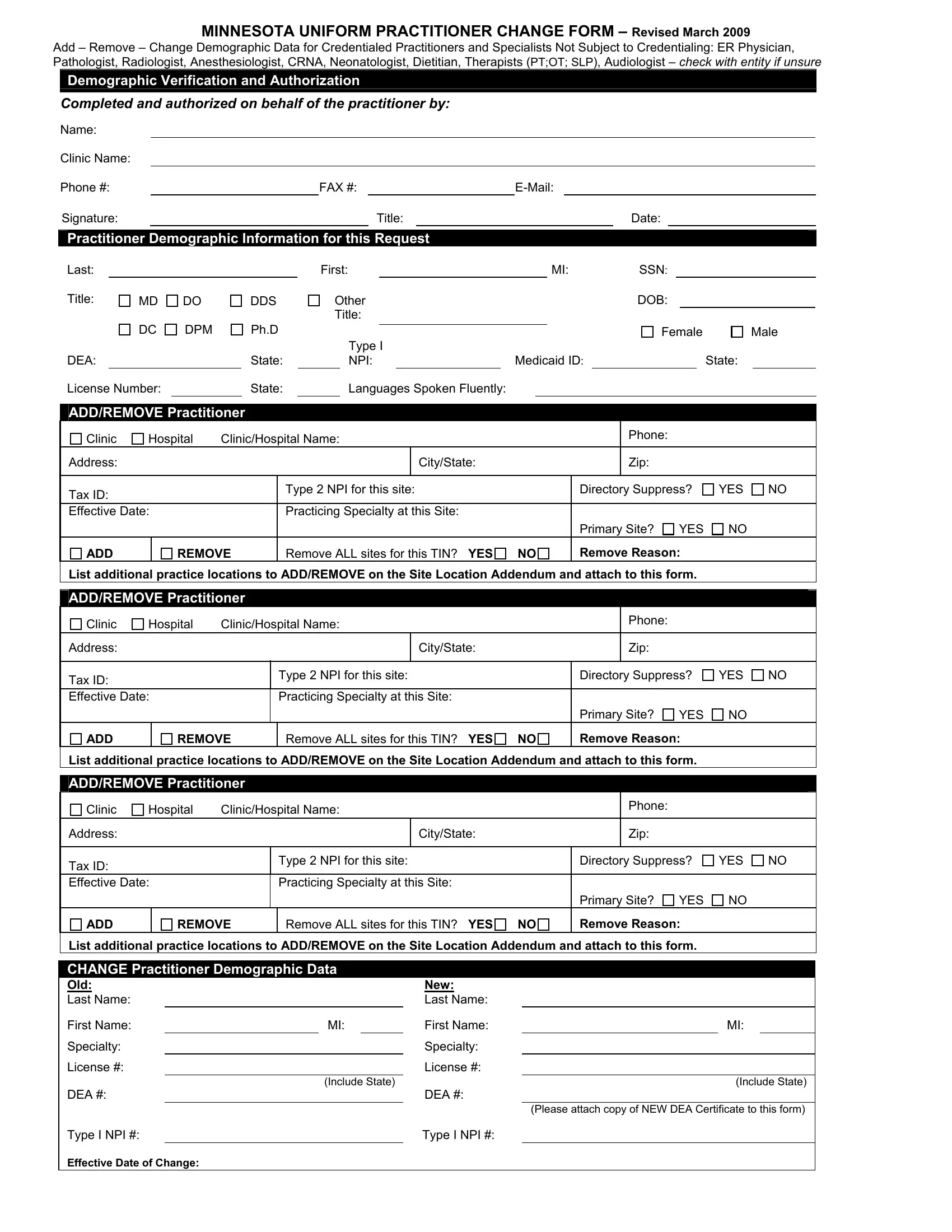
MINNESOTA UNIFORM PRACTITIONER CHANGE FORM – Revised March 2009
Add – Remove – Change Demographic Data for Credentialed Practitioners and Specialists Not Subject to Credentialing: ER Physician, Pathologist, Radiologist, Anesthesiologist, CRNA, Neonatologist, Dietitian, Therapists (PT;OT; SLP), Audiologist – check with entity if unsure
Demographic Verification and Authorization
Completed and authorized on behalf of the practitioner by:
Name:
Clinic Name:
Phone #: |
|
FAX #: |
|||||||
Signature: |
|
|
|
Title: |
|
|
|
Date: |
|
Practitioner Demographic Information for this Request
Last: |
|
|
|
First: |
|
|
|
MI: |
SSN: |
||
Title: |
MD |
DO |
DDS |
Other |
|
|
|
DOB: |
|||
|
|
|
|
Title: |
|
|
|
|
|
||
|
DC |
DPM |
Ph.D |
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
Type I |
|
|
|
|
|
|
DEA: |
|
|
State: |
|
NPI: |
|
Medicaid ID: |
|
State: |
||
Male
License Number: |
|
State: |
|
Languages Spoken Fluently: |
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
|
|
|
|
|
|
|
|
ADD |
REMOVE |
Remove ALL sites for this TIN? YES NO |
Remove Reason: |
||||
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
|
|
|
|
|
|
|
|
ADD |
REMOVE |
Remove ALL sites for this TIN? YES NO |
Remove Reason: |
||||
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
CHANGE Practitioner Demographic Data
Old: |
|
|
New: |
|
|
|
|
Last Name: |
|
|
|
Last Name: |
|
|
|
First Name: |
|
MI: |
|
First Name: |
|
MI: |
|
Specialty: |
|
|
|
Specialty: |
|
|
|
License #: |
|
|
License #: |
|
|
|
|
|
|
(Include State) |
|
|
(Include State) |
||
DEA #: |
|
|
DEA #: |
|
|
|
|
|
|
|
|
|
(Please attach copy of NEW DEA Certificate to this form) |
||
Type I NPI #: |
|
|
|
Type I NPI #: |
|
|
|
Effective Date of Change: |
|
|
|
|
|
|
|
THE FOLLOWING SITE LOCATION ADDENDUM FORM IS USED IN CONJUNCTION WITH THE MINNESOTA UNIFORM PRACTITIONER CHANGE FORM WHEN ADDING OR REMOVING PRACTITIONERS FROM MORE THAN THREE SITES. THIS FORM WILL ONLY BE ACCEPTED WHEN IT IS ACCOMPANIED BY A COMPLETED MINNESOTA UNIFORM PRACTITIONER CHANGE FORM.
SITE LOCATION ADDENDUM
Must indicate if the additional site(s) are being ADDED or REMOVED
ADDITIONAL LOCATION(s) FOR:
Last: |
|
First: |
|
MI: |
|
SSN: |
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
|
|
|
|
|
|
|
|
|
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
||||
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
ADD/REMOVE Practitioner
Clinic |
Hospital |
Clinic/Hospital Name: |
||
Address: |
|
|
|
City/State: |
|
|
|
|
|
Tax ID: |
|
|
Type 2 NPI for this site: |
|
|
|
|
|
|
Effective Date: |
|
Practicing Specialty at this Site: |
||
YES NO
ADD |
REMOVE |
Remove ALL sites for this TIN? YES |
NO |
Remove Reason: |
List additional practice locations to ADD/REMOVE on the Site Location Addendum and attach to this form.
Location addendum.doc – March 2009