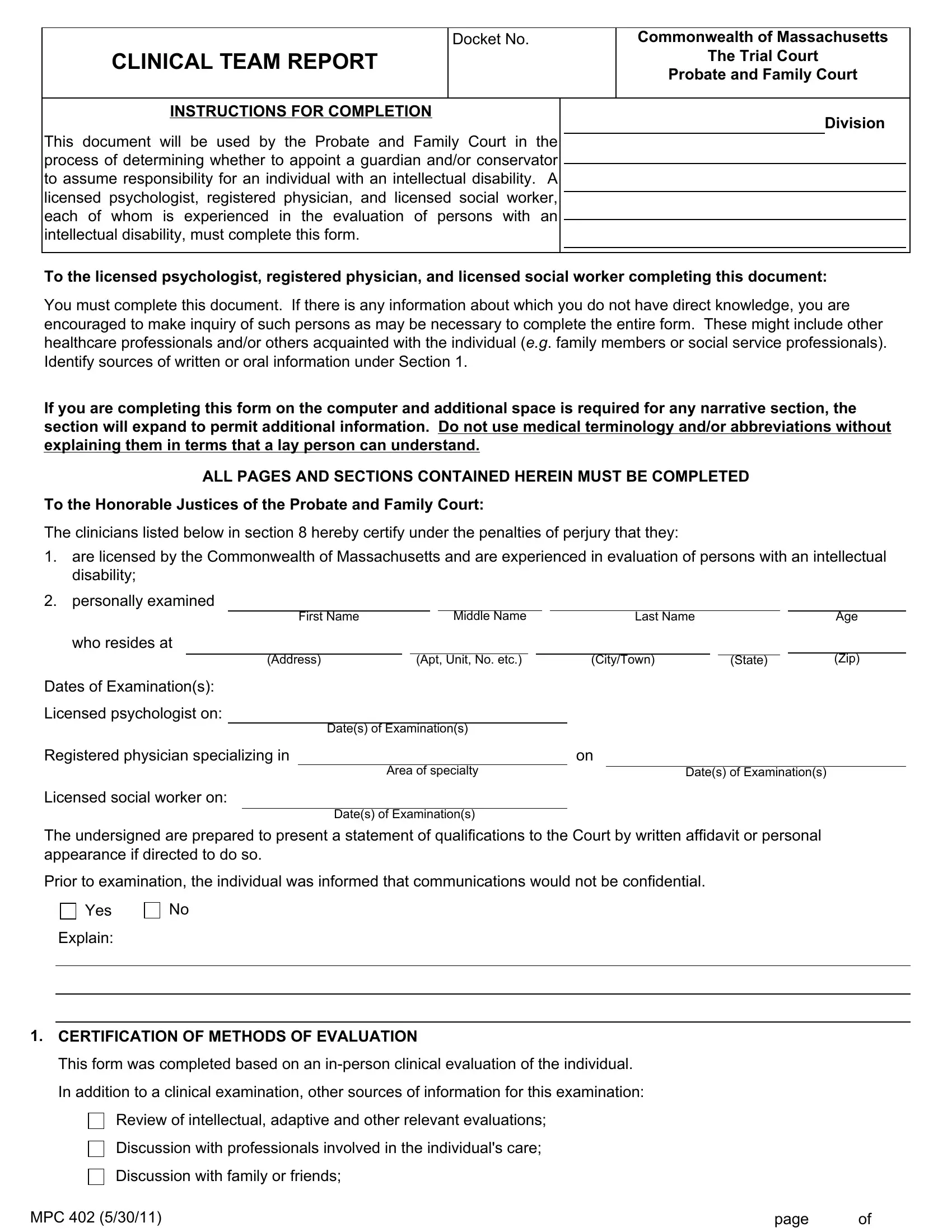

Working with PDF documents online is definitely a piece of cake with our PDF editor. Anyone can fill in mass probate courforms clinical team report here and try out a number of other options we provide. FormsPal is devoted to providing you the absolute best experience with our tool by constantly adding new functions and upgrades. With all of these updates, using our tool gets easier than ever before! Here is what you'll have to do to get going:
Step 1: Open the PDF inside our tool by pressing the "Get Form Button" above on this webpage.
Step 2: This tool gives you the opportunity to change PDF documents in many different ways. Change it by writing customized text, adjust original content, and place in a signature - all possible in minutes!
This PDF form will require specific information; to guarantee consistency, please make sure to pay attention to the guidelines below:
1. The mass probate courforms clinical team report needs specific details to be entered. Ensure that the next blank fields are completed:
2. Your next stage is usually to submit these blanks: who resides at, Dates of Examinations, Licensed psychologist on, First Name, Middle Name, Last Name, Address, Apt Unit No etc, CityTown, State, Age, Zip, Dates of Examinations, Registered physician specializing, and Area of specialty.
When it comes to State and Zip, be sure you do everything right in this section. Both of these are thought to be the key ones in this form.
3. The next segment is quite straightforward, In addition to a clinical, Review of intellectual adaptive, Discussion with professionals, Discussion with family or friends, MPC, and page - all these empty fields needs to be filled out here.

4. The following section comes next with these particular empty form fields to look at: Other, Names and titlesrelationships of, Name, TitleRelationship to individual, List any intellectual adaptive or, Test, Date, State numerical result for IQ test, CLINICALLY DIAGNOSED CONDITIONS, Intellectual Disability, Diagnosis of Intellectual, and Does the individual have an.
5. Now, this final segment is what you will need to complete before closing the document. The fields at issue are the following: Does the individual have an, Yes, List diagnosis and describe level, B Other Relevant Diagnoses List, C List all Medications that may, Name of medicationdosageschedule, Describe any positive or negative, and on the individuals ability to make.
Step 3: After you have reread the details in the file's blanks, press "Done" to conclude your form at FormsPal. Try a 7-day free trial plan at FormsPal and obtain immediate access to mass probate courforms clinical team report - with all adjustments kept and accessible inside your personal cabinet. We do not share or sell the details that you type in while working with documents at FormsPal.