
mssp referral form can be completed easily. Simply use FormsPal PDF editing tool to get it done right away. FormsPal is committed to providing you with the perfect experience with our editor by continuously presenting new functions and enhancements. With all of these improvements, using our editor becomes easier than ever before! All it requires is just a few easy steps:
Step 1: Click on the "Get Form" button at the top of this webpage to open our tool.
Step 2: The editor allows you to change nearly all PDF documents in a variety of ways. Enhance it by adding any text, correct what's originally in the file, and put in a signature - all readily available!
Be attentive when filling out this document. Make sure that every blank is filled out properly.
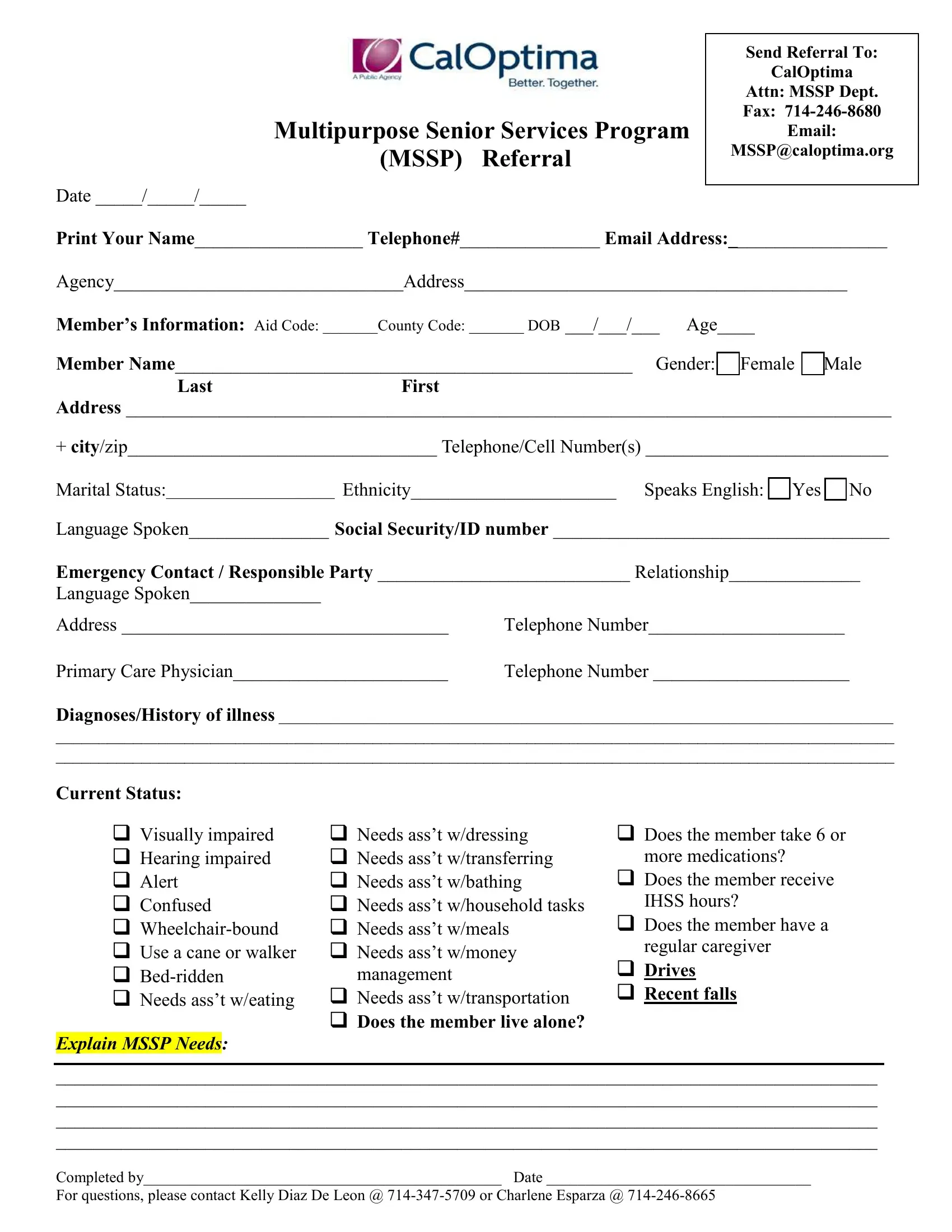
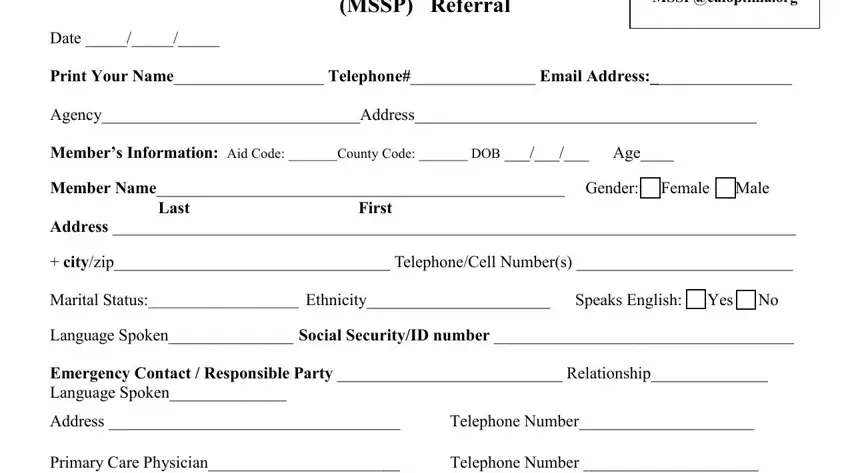
1. You will want to fill out the mssp referral form properly, so take care when filling in the segments comprising all of these blank fields:
2. Your next stage is to complete these blanks: DiagnosesHistory of illness, Current Status, Visually impaired Hearing, Needs asst wdressing Needs asst, management, Needs asst wtransportation Does, Does the member take or, more medications, Does the member receive, IHSS hours, Does the member have a, regular caregiver, Drives Recent falls, and Explain MSSP Needs.
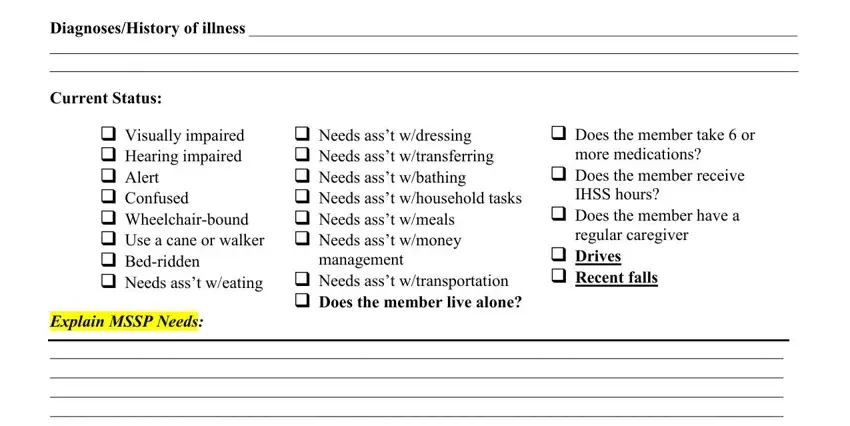
When it comes to Needs asst wtransportation Does and Does the member take or, make sure you don't make any errors here. Both these are surely the key fields in the form.
Step 3: As soon as you have reread the details in the fields, simply click "Done" to complete your FormsPal process. After starting afree trial account at FormsPal, you'll be able to download mssp referral form or email it right off. The PDF will also be readily accessible from your personal account with all your modifications. Whenever you work with FormsPal, it is simple to complete documents without worrying about data breaches or records getting distributed. Our secure software helps to ensure that your private data is maintained safely.