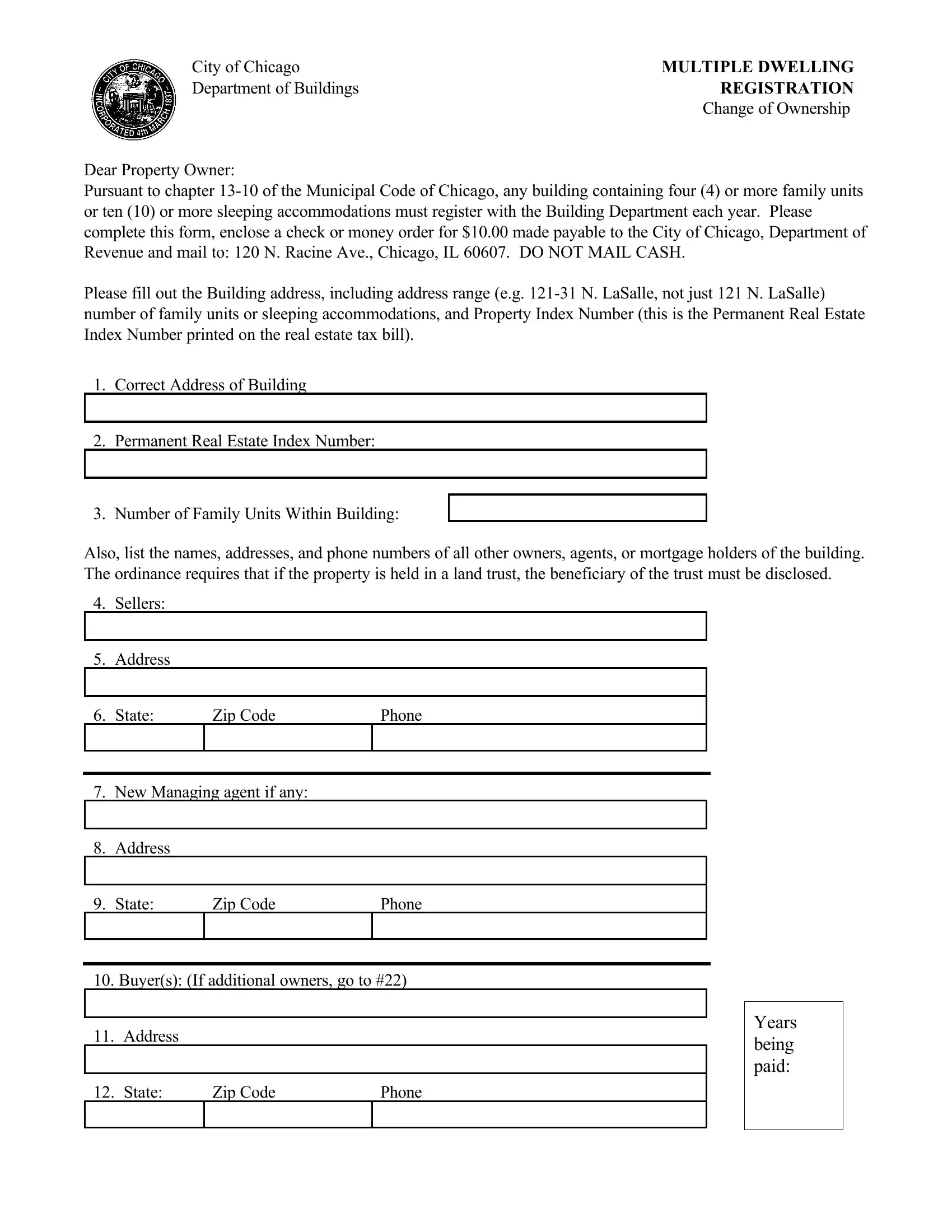
In the bustling metropolis of Chicago, where the skyline is dotted with an array of multi-family dwellings and accommodations designed for varied living arrangements, the Multiple Dwelling Registration form emerges as a crucial document for property owners. Crafted under the auspices of the Department of Buildings, this form serves as a testament to the city's commitment to maintaining an up-to-date record of its diverse architectural habitats. Per Chapter 13-10 of the Municipal Code of Chicago, proprietors of buildings that house four or more family units, or provide ten or more sleeping accommodations, find themselves navigating the annual requirement of registration. A modest fee of $10.00, payable to the City of Chicago, Department of Revenue, accompanies the submission of this form to an address specified for this purpose. The form intricately demands details such as the exact address of the building, inclusive of any range it might span, alongside the Permanent Real Estate Index Number—a unique identifier mirroring those found on real estate tax bills. It further delves into the quantification of family units or sleeping accommodations within said premises. The ordinance meticulously extends its reach to cover the disclosure of names, addresses, and contact numbers of all entities associated with the ownership, management, or financial backing of the building, ensuring a comprehensive capture of information. This requirement stretches to include details of any land trust beneficiaries, underscoring the city’s endeavor to foster transparency and accountability in property management and ownership. Thus, serving as a bridge between property stewards and the city’s regulatory framework, the Multiple Dwelling Registration form embeds itself as a pivotal instrument in the orchestration of urban living spaces.
| Question | Answer |
|---|---|
| Form Name | Multiple Dwelling Registration Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | chicago multiple registration ownership, chicago dwelling change download, chicago multiple dwelling, chicago multiple dwelling registration |
City of Chicago |
MULTIPLE DWELLING |
Department of Buildings |
REGISTRATION |
|
Change of Ownership |
Dear Property Owner:
Pursuant to chapter
Please fill out the Building address, including address range (e.g.
1.Correct Address of Building
2.Permanent Real Estate Index Number:
3. Number of Family Units Within Building:
Also, list the names, addresses, and phone numbers of all other owners, agents, or mortgage holders of the building. The ordinance requires that if the property is held in a land trust, the beneficiary of the trust must be disclosed.
4.Sellers:
5.Address
|
|
|
|
6. State: |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
7.New Managing agent if any:
8.Address
|
|
|
|
9. State: |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
10.Buyer(s): (If additional owners, go to #22)
11.Address
|
|
|
12. State: |
Zip Code |
Phone |
|
|
|
Years being paid:
13.Trust Beneficiary:
14.Address:
15. State |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
16.Office or Responsible Partner:
17.Address:
18. State |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
19.Mortgage Holder
20.Address:
21. State |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
22.Additional Owners(s) (For more owners, attach separate sheet)
23.Address:
24. State |
Zip Code |
Phone |
|
|
|
|
|
|
|
|
|
Signature to verify that the information on this form is correct:
Name |
Date |
Years being paid: