Municipal Form No. 103 |
(To be accomplished in quadruplicate) |
REMARKS/ANNOTATION |
(Revised January 1993) |
|
|
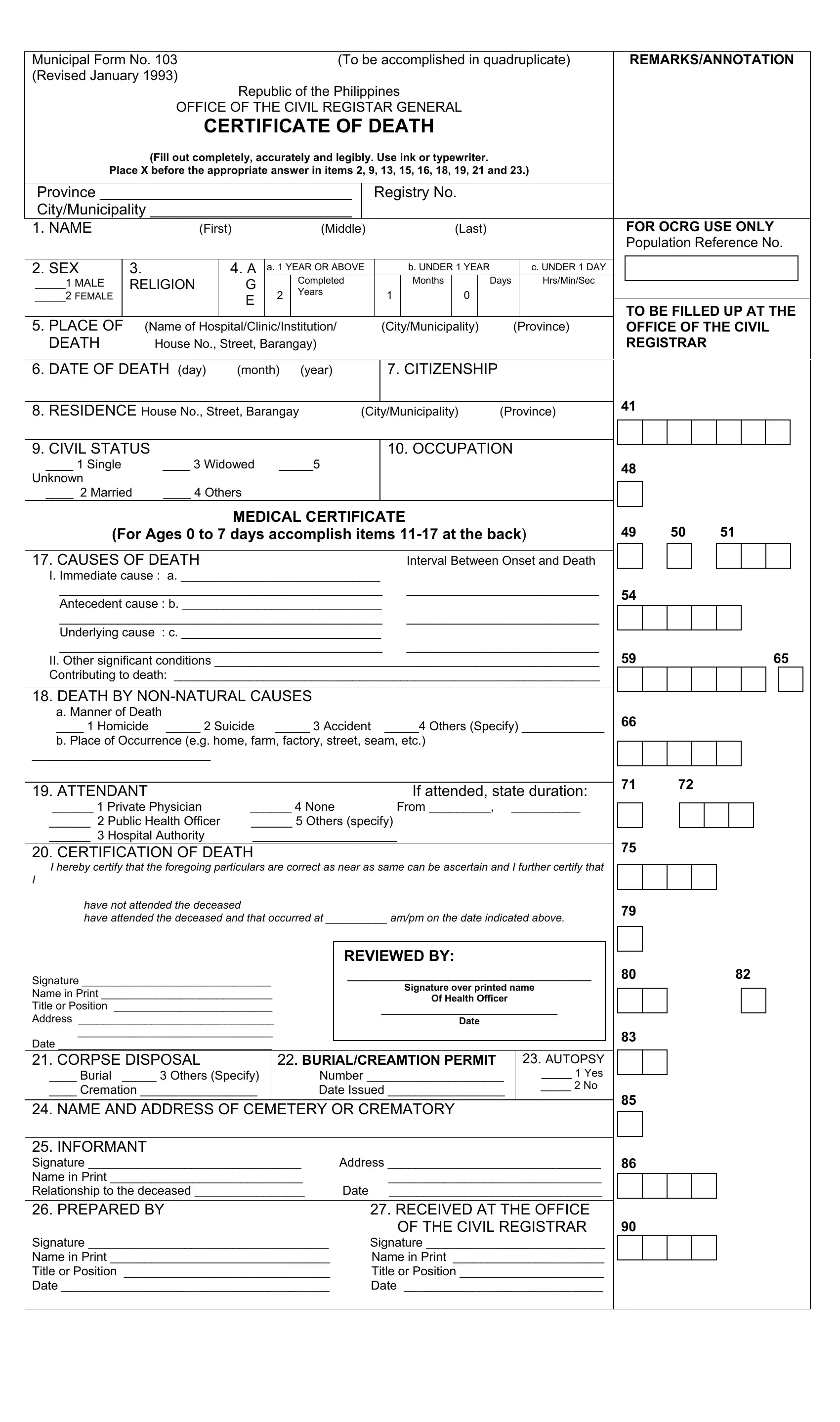
Republic of the Philippines
OFFICE OF THE CIVIL REGISTAR GENERAL
CERTIFICATE OF DEATH
(Fill out completely, accurately and legibly. Use ink or typewriter.
Place X before the appropriate answer in items 2, 9, 13, 15, 16, 18, 19, 21 and 23.)
Province ______________________________ |
|
|
Registry No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City/Municipality ________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. NAME |
|
(First) |
|
|
(Middle) |
|
|
|
|
|
(Last) |
|
|
|
|
|
|
|
FOR OCRG USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Population Reference No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. SEX |
3. |
|
|
4. A |
a. 1 YEAR OR ABOVE |
|
|
|
|
b. UNDER 1 YEAR |
|
|
c. UNDER 1 DAY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____1 MALE |
RELIGION |
|
G |
|
|
Completed |
|
|
|
|
Months |
|
|
Days |
|
|
Hrs/Min/Sec |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
Years |
|
|
|
|
|
1 |
|
|
0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____2 FEMALE |
|
|
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE FILLED UP AT THE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. PLACE OF |
(Name of Hospital/Clinic/Institution/ |
|
|
|
|
(City/Municipality) |
(Province) |
|
|
OFFICE OF THE CIVIL |
DEATH |
|
House No., Street, Barangay) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REGISTRAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. DATE OF DEATH (day) |
(month) |
(year) |
|
|
|
|
|
7. CITIZENSHIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
41 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. RESIDENCE House No., Street, Barangay |
(City/Municipality) |
|
(Province) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. CIVIL STATUS |
|
|
|
|
|
|
|
|
|
|
|
|
10. OCCUPATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ 1 Single |
|
____ 3 Widowed |
_____5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
48 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Unknown |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ 2 Married |
____ 4 Others |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL CERTIFICATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(For Ages 0 to 7 days accomplish items 11-17 at the back) |
49 |
50 |
|
|
51 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. CAUSES OF DEATH |
|
|
|
|
|
|
|
|
|
|
|
Interval Between Onset and Death |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I. Immediate cause : a. _____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_______________________________________________ |
____________________________ |
|
|
54 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Antecedent cause : b. _____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_______________________________________________ |
____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Underlying cause : c. _____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_______________________________________________ |
____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
II. Other significant conditions ________________________________________________________ |
59 |
|
|
|
|
|
65 |
|
|
|
Contributing to death: ______________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. DEATH BY NON-NATURAL CAUSES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. Manner of Death |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
66 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ 1 Homicide |
_____ 2 Suicide |
|
_____ 3 Accident |
_____4 Others (Specify) ____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Place of Occurrence (e.g. home, farm, factory, street, seam, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
71 |
72 |
|
|
|
|
|
|
|
|
|
|
19. ATTENDANT |
|
|
|
|
|
|
|
|
|
|
|
|
|
If attended, state duration: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
______ 1 Private Physician |
______ 4 None |
|
|
|
|
|
From _________, |
__________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
______ 2 Public Health Officer |
______ 5 Others (specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
______ 3 Hospital Authority |
_____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. CERTIFICATION OF DEATH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
75 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I hereby certify that the foregoing particulars are correct as near as same can be ascertain and I further certify that |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
have not attended the deceased |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
79 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
have attended the deceased and that occurred at __________ am/pm on the date indicated above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REVIEWED BY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature _______________________________ |
|
|
_____________________________ |
|
|
80 |
|
|
|
|
|
82 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature over printed name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name in Print ____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Of Health Officer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title or Position __________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address ________________________________ |
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
83 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date ___________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. CORPSE DISPOSAL |
|
|
22. BURIAL/CREAMTION PERMIT |
|
|
23. AUTOPSY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ Burial _____ 3 Others (Specify) |
|
|
Number ____________________ |
|
|
_____ 1 Yes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
____ Cremation _________________ |
|
|
Date Issued _________________ |
|
|
_____ 2 No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
85 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. NAME AND ADDRESS OF CEMETERY OR CREMATORY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25. INFORMANT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature _______________________________ |
Address _______________________________ |
86 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name in Print ____________________________ |
|
|
|
|
|
_______________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relationship to the deceased ________________ |
Date |
|
|
|
_______________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26. PREPARED BY |
|
|
|
|
|
|
|
27. RECEIVED AT THE OFFICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF THE CIVIL REGISTRAR |
90 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature ___________________________________ |
|
|
Signature __________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name in Print ________________________________ |
|
|
Name in Print ______________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title or Position |
______________________________ |
|
|
|
Title or Position _____________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date _______________________________________ |
|
|
Date _____________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR AGES 0 TO 7 DAYS |
|
|
|
11. DATE OF BIRTH |
12. AGE OF THE MOTHER |
13.METHOD OF DELIVERY |
(day) |
(month) (year) |
|
___ 1 Normal; Spontaneous vertex |
|
|
|
___ 2 Other (Specify) |
|
|
|
______________________ |
14. LENGTH OF PREGNANCY: |
____________ competed weeks |
15. TYPE OF BIRTH |
16. IF MULTIPLE BIRTH, CHILD WAS |
__ 1 Single ___ 2 Twin ___ 3 Triplet, etc. |
___ 1 First |
___ 2 Second |
___ 3 Others (Specify) |
|
|
|
|
MEDICAL CERTIFICATE
11. CAUSES OF DEATH
a. Main disease/condition of infant ______________________________________________________________________
b. Other diseases/conditions of infant ____________________________________________________________________
c. Main maternal disease/condition affecting infant _________________________________________________________
d. Other maternal disease/condition affecting infant _________________________________________________________
e. Other relevant circumstances ________________________________________________________________________
CONTINUE FILL UP ITEM 18
POSTMORTEM CERTIFICATE OF DEATH
I HEREBY CERTIFY that I have this ________ day of ______________, ____________ performed an autopsy
upon the body of the deceased and that the cause of death was as follows: _______________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
Signature __________________________ |
Title/Designation ______________________ |
Name in Print _______________________ |
Address ____________________________ |
|
___________________________________ |
|
|
CERTIFICATION OF EMBALMER |
I HEREBY CERTIFY that I have embalmed ________________________________________________ after having |
followed all the regulations prescribed by the Department of Health. |
|
Signature __________________________ |
Title/Designation _____________________ |
Name in Print _______________________ |
License No. _________________________ |
Address ___________________________ |
Issued on __________ at ______________ |
__________________________________ |
Expiry Date _________________________ |
|
|
Republic of the Philippines _________________________________ |
) |
Province of _____________________________________________ |
)S.S. |
City / Municipality of ______________________________________ |
) |
AFFIDAVIT FOR DELAYED REGISTRATION OF DEATH
I, ________________________________________________, of legal age, single/married, after
being duly sworn to in accordance with law, do hereby depose and say:
1.That ____________________________________ died on ___________________________ in
_____________________________________________________ and was burried/cremated in
_________________________________________________________ on ________________.
2.That the deceased was/was not attended to at the time of his death.
3.That the reason for the delay in registering this death was due to ________________________
____________________________________________________.
______________________________________
(Signature of Affiant)
Community Tax No. ____________________
Date Issued __________________________
Place Issued __________________________
SUBSCRIBED AND SWORN to before me this _________ day of ________________, ________________
at ___________________________________________________________________________________, Philippines.
___________________________________
_____________________________________
(Signature of Administering Officer) |
(Title/Designation) |
_______________________________________ |
___________________________________ |
(Name in Print) |
(Address) |