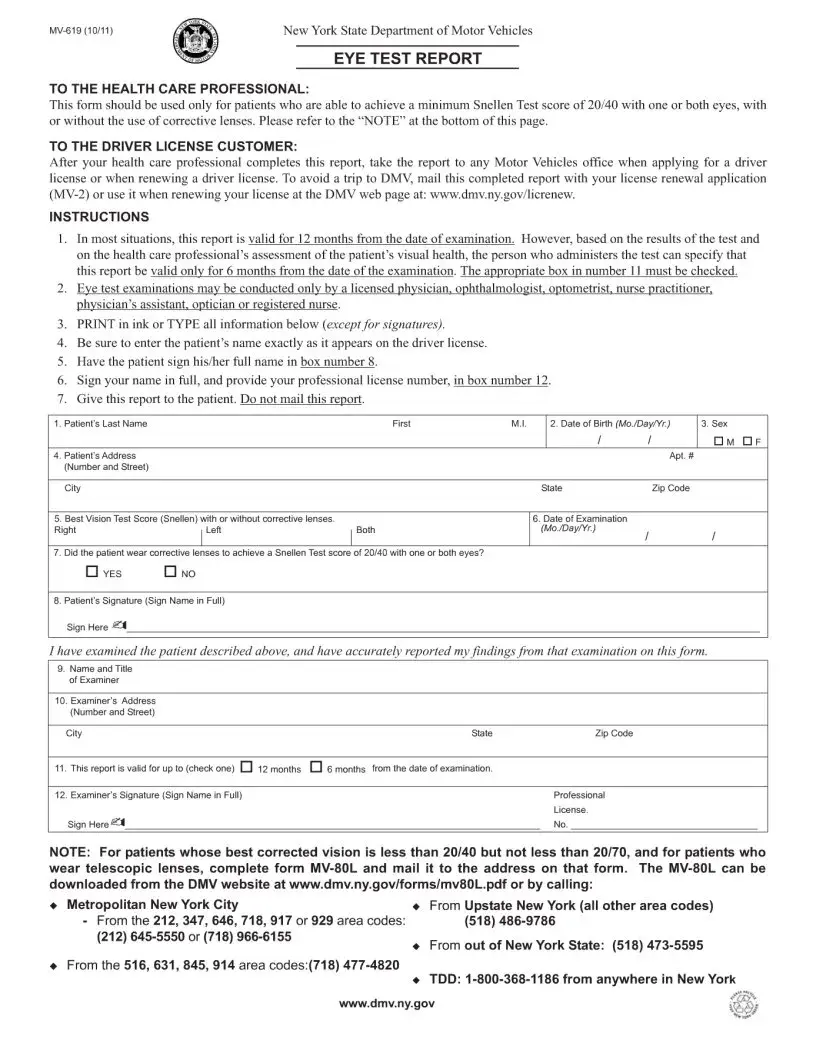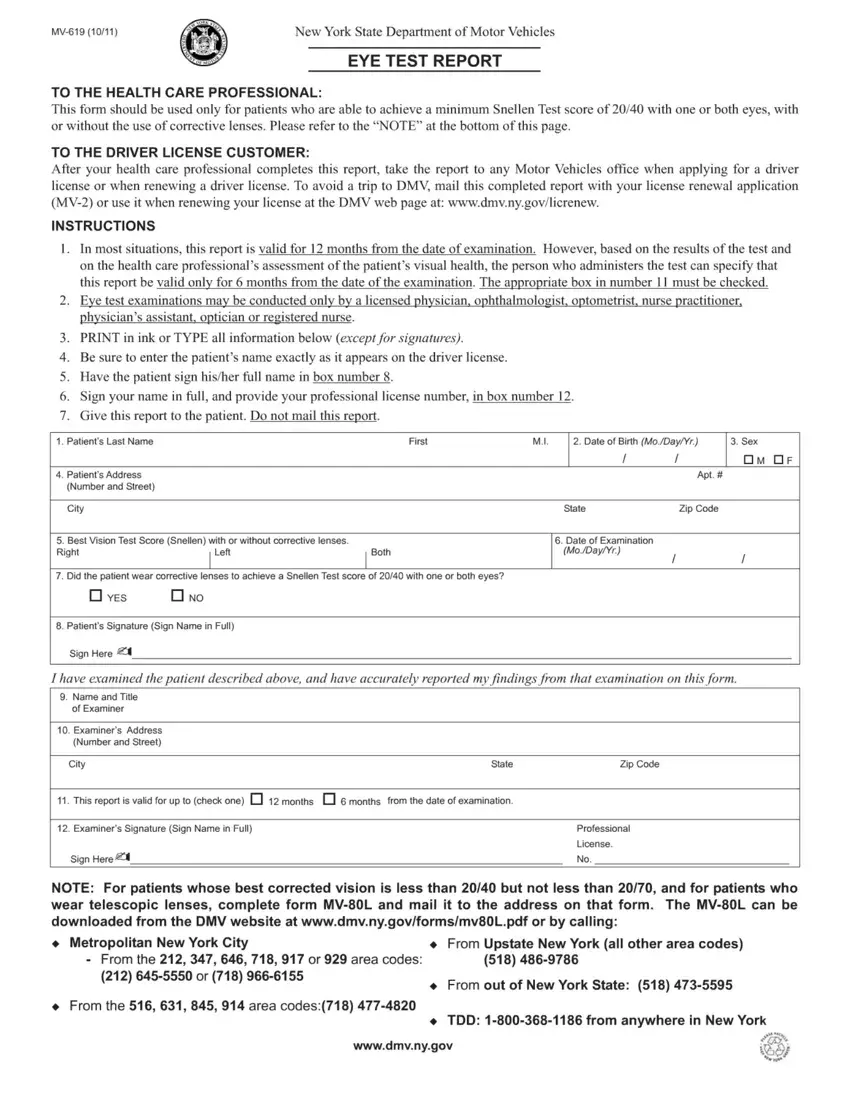
Ensuring the safety of our roads involves various measures, and one crucial aspect is making certain that drivers have the necessary visual acuity to navigate safely. This is where the DMV Eye Test 619 form plays a vital role. It's a standardized document used across many states, designed to assess an individual's vision to ensure it meets the legal requirements for operating a vehicle. The form is often a prerequisite for obtaining or renewing a driver's license and must be completed by a certified vision examiner, such as an optometrist or ophthalmologist. By measuring aspects such as visual acuity, peripheral vision, and the ability to perceive colors, the DMV Eye Test 619 form helps in identifying vision-related issues that could potentially impair a person’s driving abilities, ensuring that all drivers on the road are capable of seeing clearly and responding to conditions appropriately.
| Question | Answer |
|---|---|
| Form Name | Dmv Eye Test Form 619 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | mv 619 or form mv 619r eye test report, form mv 619, ny dmv eye, dmv eye yest |