
The idea driving our PDF editor was to help it become as easy to use as possible. You'll find the overall procedure of managing renew handicap placard pa hassle-free should you follow the following steps.
Step 1: Click the "Get Form Here" button.
Step 2: At this point, you can start editing the renew handicap placard pa. The multifunctional toolbar is at your disposal - add, eliminate, adjust, highlight, and undertake other sorts of commands with the content material in the document.
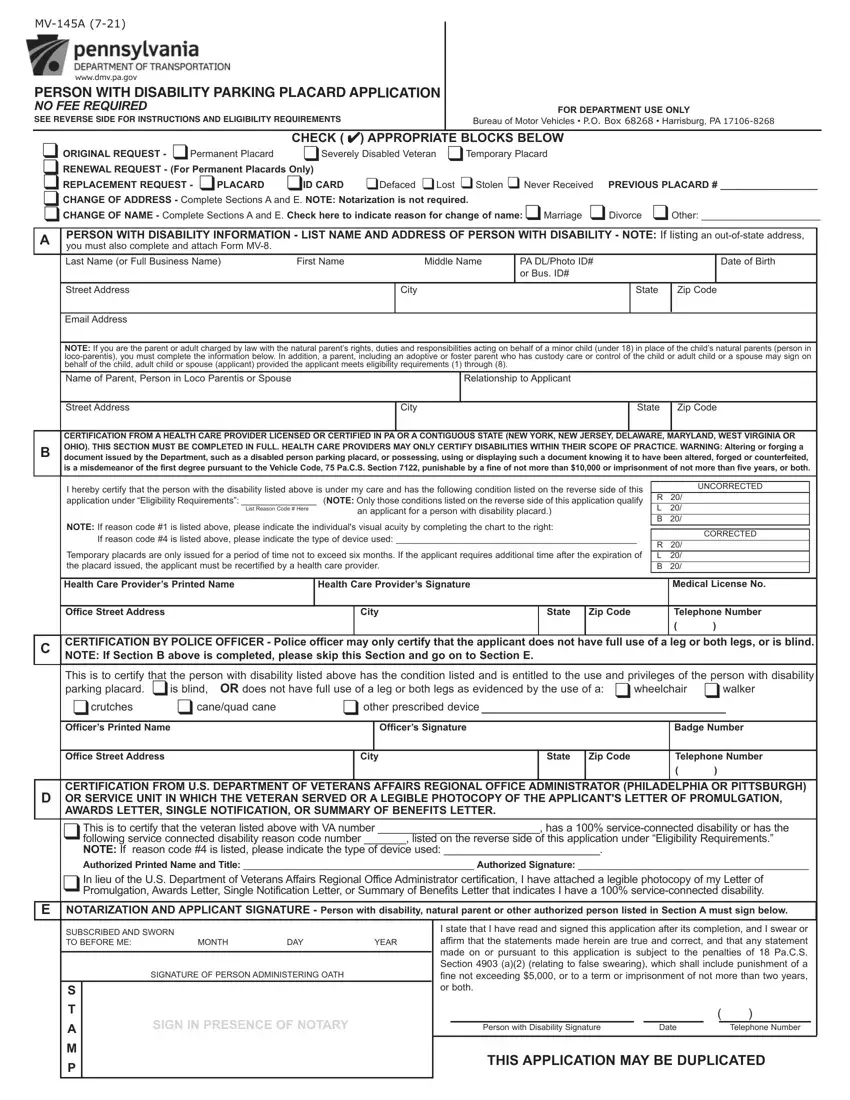
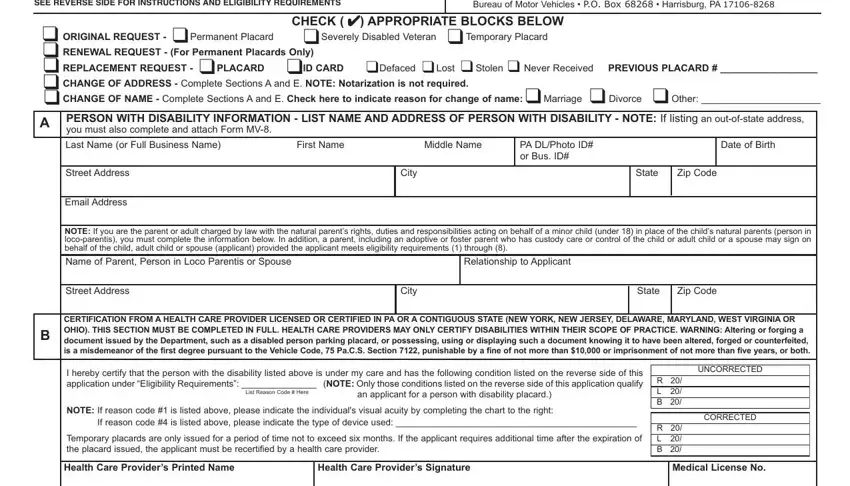
Enter the data required by the system to prepare the form.
Make sure you provide your details in the box Office Street Address, City, State, Zip Code, Telephone Number, C CERTIFICATION BY POLICE OFFICER, NOTE If Section B above is, This is to certify that the person, is blind OR does not have full use, other prescribed device, canequad cane, Officers Signature, Badge Number, wheelchair, and crutches.
Step 3: Once you've hit the Done button, your form is going to be accessible for upload to each electronic device or email address you identify.
Step 4: Ensure that you keep away from potential complications by having a minimum of 2 copies of your document.
