
When working in the online tool for PDF editing by FormsPal, you can complete or edit na form download right here. Our expert team is ceaselessly working to enhance the tool and ensure it is even easier for clients with its handy features. Uncover an constantly innovative experience now - check out and discover new possibilities along the way! This is what you will have to do to get started:
Step 1: Simply click on the "Get Form Button" above on this webpage to launch our pdf form editing tool. This way, you will find everything that is needed to work with your document.
Step 2: With the help of this handy PDF editor, you're able to accomplish more than just complete blanks. Edit away and make your docs seem perfect with customized text added in, or adjust the file's original input to perfection - all comes along with an ability to insert your own graphics and sign the PDF off.
This document will need particular data to be filled out, thus be sure you take whatever time to enter what is required:
1. When filling out the na form download, ensure to complete all of the important fields within its associated part. This will help hasten the work, which allows your information to be handled quickly and accurately.
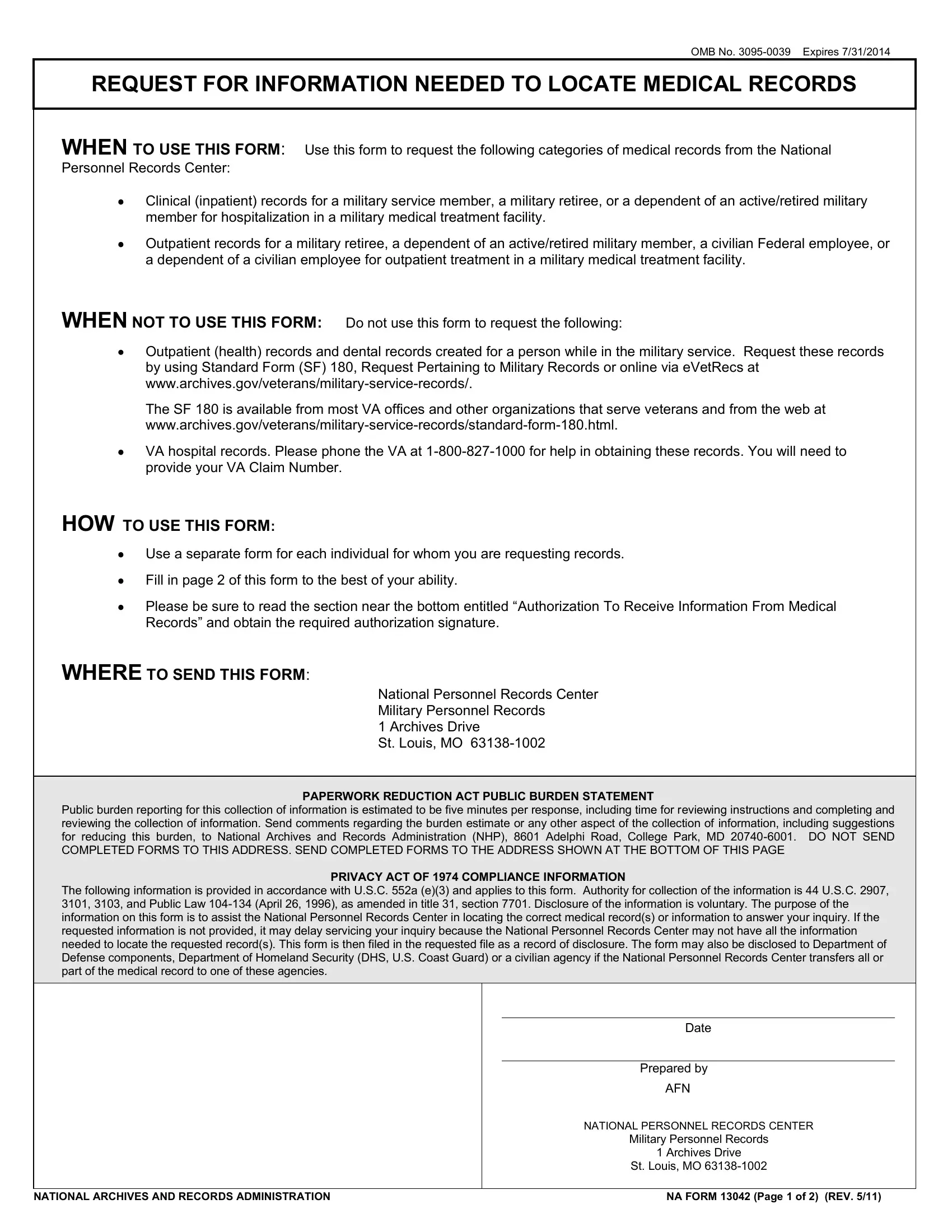
2. Your next stage is to fill in these particular blank fields: The following information is, Date, Prepared by, AFN, NATIONAL PERSONNEL RECORDS CENTER, Military Personnel Records, Archives Drive, St Louis MO, and NATIONAL ARCHIVES AND RECORDS.
3. In this part, review SECTION I ABOUT THE PATIENT, NAME OF PATIENT at time of, Last, First, Middle Initial, A STATUS OF PATIENT AT TIME OF, MILITARY SERVICE, MEMBER, Branch of service, Service number, SSN, RETIRED MILITARY Branch of service, Service number, SSN, and Name last first middle initial. Every one of these have to be taken care of with highest accuracy.
4. All set to complete the next portion! In this case you have these SECTION II RETURN ADDRESS AND, REQUESTER IS, Patient identified in SectionA, AUTHORIZATION SIGNATURE REQUIRED, Signature of patient next of kin, Email address, Date, Next of kin of deceased patient, Show relationship, Other specify, SEND INFORMATIONDOCUMENTS TO, Name, Street, City State ZIP Code, and Daytime phone number including empty form fields to fill out.
Always be very careful when filling in Date and Patient identified in SectionA, as this is the section where most people make mistakes.
Step 3: Before moving on, make certain that all blanks have been filled out the right way. Once you are satisfied with it, press “Done." Join us now and immediately get access to na form download, prepared for download. Each modification you make is handily kept , letting you edit the document further when required. We don't share any details that you type in while filling out forms at FormsPal.