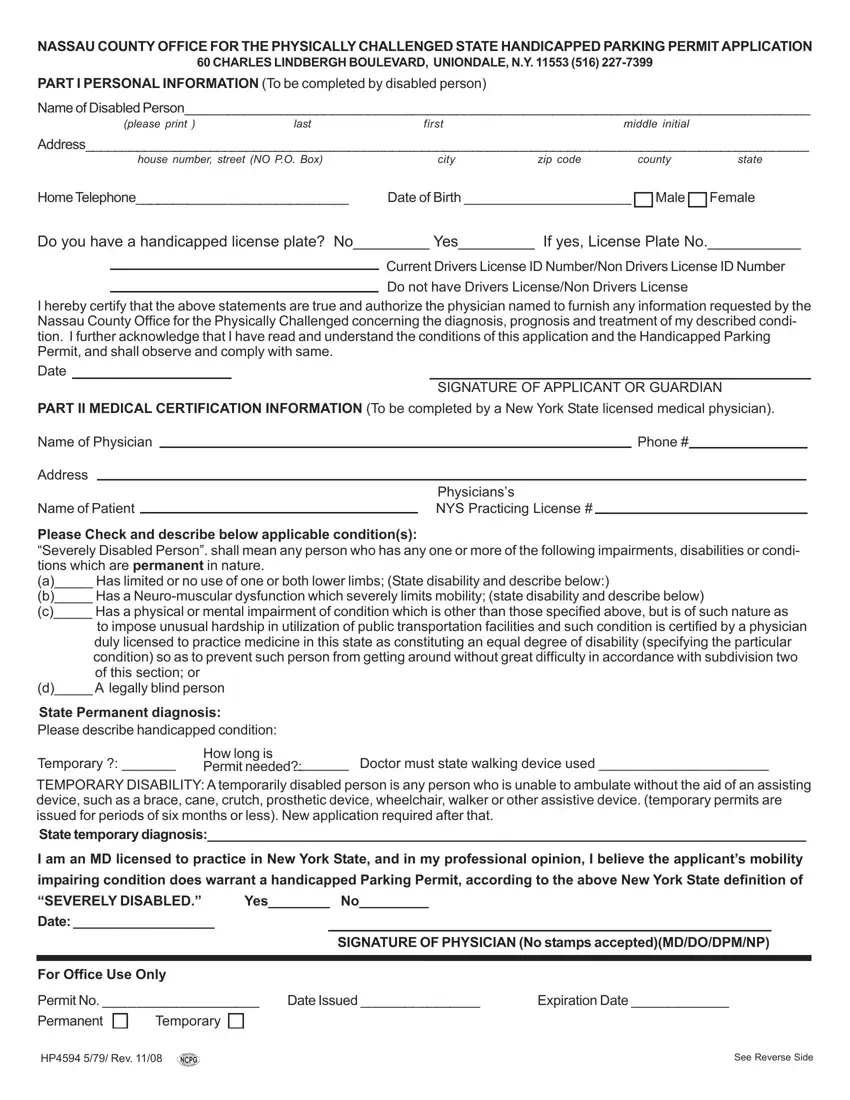
NASSAU COUNTY OFFICE FOR THE PHYSICALLY CHALLENGED STATE HANDICAPPED PARKING PERMIT APPLICATION
60 CHARLES LINDBERGH BOULEVARD, UNIONDALE, N.Y. 11553 (516) 227-7399
PART I PERSONAL INFORMATION (To be completed by disabled person)
Name of Disabled Person_____________________________________________________________________________________
(please print )lastfirstmiddle initial
Address___________________________________________________________________________________________________
house number, street (NO P.O. Box) |
city |
zip code |
county |
state |
HomeTelephone_____________________________ |
Date of Birth ______________________ |
Male |
Female |
Do you have a handicapped license plate? No_________ Yes_________ If yes, License Plate No.___________
Current Drivers License ID Number/Non Drivers License ID Number Do not have Drivers License/Non Drivers License
I hereby certify that the above statements are true and authorize the physician named to furnish any information requested by the Nassau County Office for the Physically Challenged concerning the diagnosis, prognosis and treatment of my described condi- tion. I further acknowledge that I have read and understand the conditions of this application and the Handicapped Parking Permit, and shall observe and comply with same.
Date
SIGNATURE OF APPLICANT OR GUARDIAN
PART II MEDICAL CERTIFICATION INFORMATION (To be completed by a New York State licensed medical physician).
Name of Physician |
|
|
|
Phone # |
Address |
|
|
|
|
|
|
|
|
|
|
|
Physicians’s |
Name of Patient |
|
|
NYS Practicing License # |
|
|
Please Check and describe below applicable condition(s):
“Severely Disabled Person”. shall mean any person who has any one or more of the following impairments, disabilities or condi- tions which are permanent in nature.
(a)_____ Has limited or no use of one or both lower limbs; (State disability and describe below:)
(b)_____ Has a Neuro-muscular dysfunction which severely limits mobility; (state disability and describe below)
(c)_____ Has a physical or mental impairment of condition which is other than those specified above, but is of such nature as
to impose unusual hardship in utilization of public transportation facilities and such condition is certified by a physician duly licensed to practice medicine in this state as constituting an equal degree of disability (specifying the particular condition) so as to prevent such person from getting around without great difficulty in accordance with subdivision two of this section; or
(d)_____ A legally blind person |
|
State Permanent diagnosis: |
|
Please describe handicapped condition: |
|
Temporary ?: _______ |
How long is |
_______ Doctor must state walking device used ______________________ |
|
|
Permit needed?: |
TEMPORARY DISABILITY: A temporarily disabled person is any person who is unable to ambulate without the aid of an assisting device, such as a brace, cane, crutch, prosthetic device, wheelchair, walker or other assistive device. (temporary permits are issued for periods of six months or less). New application required after that.
State temporary diagnosis:_________________________________________________________________________________
I am an MD licensed to practice in New York State, and in my professional opinion, I believe the applicant’s mobility impairing condition does warrant a handicapped Parking Permit, according to the above New York State definition of
“SEVERELY DISABLED.” |
Yes________ No_________ |
|
|
Date: ___________________ |
|
|
|
|
|
|
|
|
SIGNATURE OF PHYSICIAN (No stamps accepted)(MD/DO/DPM/NP) |
|
|
|
|
|
|
|
|
|
|
|
|
For Office Use Only |
|
|
|
|
|
Permit No. _____________________ |
Date Issued ________________ |
Expiration Date _____________ |