
With the help of the online PDF editor by FormsPal, you'll be able to fill out or modify the naukeag online here and now. To make our editor better and simpler to work with, we consistently develop new features, bearing in mind suggestions from our users. With a few simple steps, you are able to begin your PDF journey:
Step 1: Hit the "Get Form" button at the top of this page to access our tool.
Step 2: Once you access the PDF editor, you will find the document prepared to be filled in. Apart from filling out different blanks, you may also perform various other things with the form, specifically putting on your own textual content, modifying the initial textual content, adding graphics, signing the PDF, and more.
It really is straightforward to complete the pdf using this practical tutorial! Here's what you have to do:
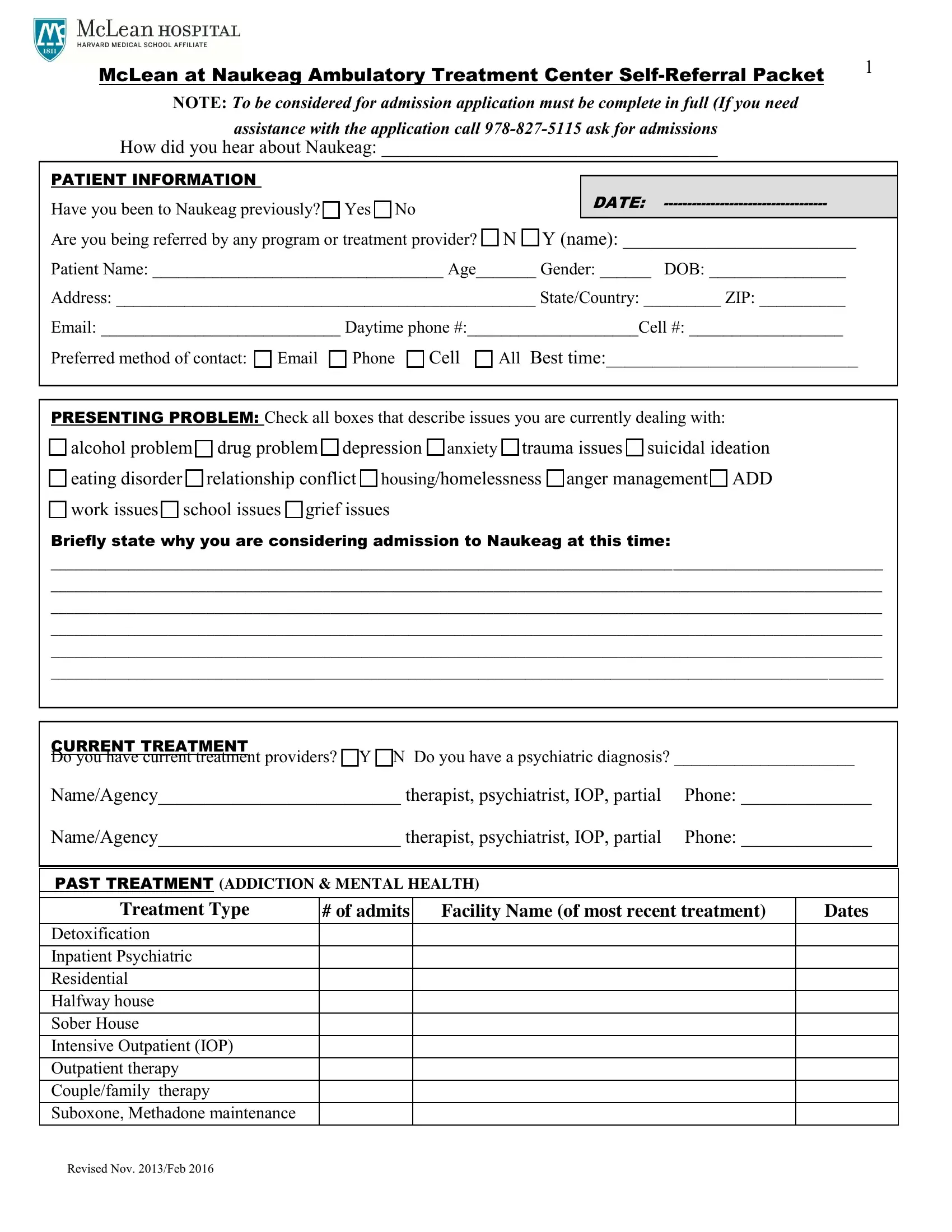
1. When filling out the the naukeag online, make sure to incorporate all needed fields within the relevant area. It will help facilitate the work, allowing for your details to be handled quickly and correctly.
2. Right after filling out the previous section, head on to the next stage and complete the necessary details in all these blanks - Briefly state why you are, C URRENT TREATMENT D o you have, Na meAgency therapist psychiatrist, Do you attend self help Meetings, PAST TREATMENT ADDICTION MENTAL, Treatment Type, of admits, Facility Name of most recent, Dates, and Detoxification Inpatient.
3. Completing Detoxification Inpatient, and Revised Nov Feb is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. Your next paragraph will require your information in the subsequent places: McLean at Naukeag Ambulatory, PATIENT NAME, DRUG USE HISTORY, Primary Drugs Secondary cid if, Frequency, Amount, Drug, Age, First Use, Last Use, Alcohol, Amphetamines, Benzodiazepines Klonopin Xanax, Cocaine, and Fentanyl. Remember to fill out all of the requested info to go further.
As to Amount and Drug, be certain you take a second look here. Those two are considered the most important fields in this document.
5. The last section to conclude this form is pivotal. Make sure that you fill in the mandatory fields, including Hallucinogens mushrooms LSD PCP DXM, Heroin, Inhalants, Ketamine, Marijuana, MDMA Ecstasy, Methadone, Methamphetamine, Morphine, Over the counter cough syrup, Oxycontin Oxycodone Percocet, Rohypnol, Steroids Anabolic, and Suboxone, prior to using the form. Or else, it can result in an unfinished and possibly invalid paper!
Step 3: After going through your fields you've filled in, press "Done" and you're done and dusted! Go for a 7-day free trial plan with us and gain instant access to the naukeag online - which you'll be able to then use as you want in your FormsPal cabinet. FormsPal guarantees your data confidentiality via a secure system that never saves or shares any sort of private information used in the PDF. Rest assured knowing your documents are kept safe whenever you use our services!