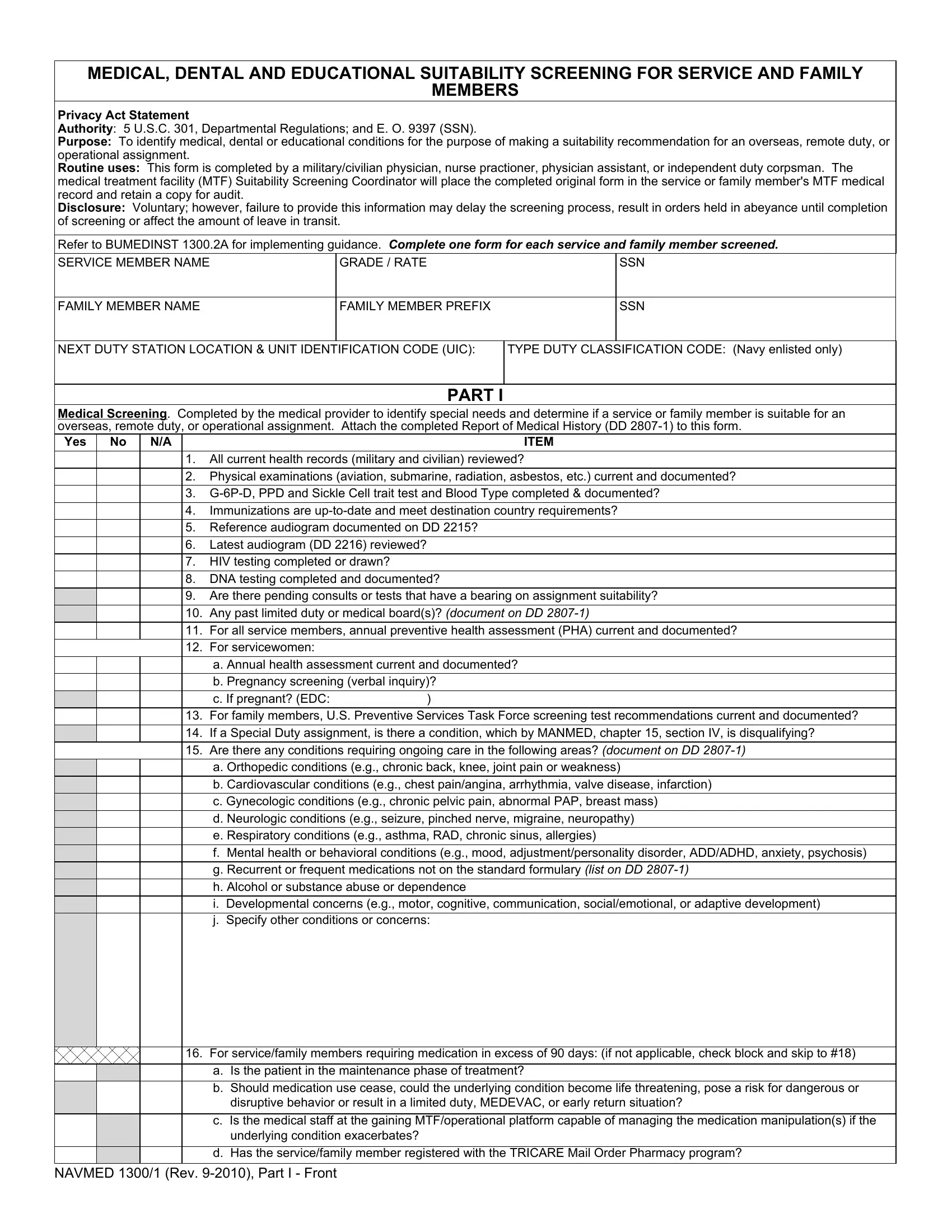
The NAVMED 1300 form is an essential document used in the United States Navy, serving a crucial role in assessing the medical, dental, and educational suitability of service members and their families for overseas, remote duty, or operational assignments. Mandated by 5 U.S.C. 301, Departmental Regulations, and Executive Order 9397 (SSN), the form facilitates a comprehensive screening process to identify any medical, dental, or educational conditions that might influence the suitability recommendation for such assignments. This rigorous screening is conducted by qualified professionals including military/civilian physicians, nurse practitioners, physician assistants, or independent duty corpsmen. These professionals ensure that the form, along with the attached Report of Medical History (DD 2807-1), thoroughly documents a variety of assessments - from reviewing all current health and dental records to validating the completion of crucial tests such as HIV, DNA, and immunizations that meet destination country requirements. Additionally, it addresses the need for special medical supplies, adaptive equipment, and the potential requirement for ongoing care in areas encompassing orthopedic, cardiovascular, gynecologic, neurologic, respiratory conditions, and more. The NAVMED 1300 form also incorporates a detailed dental screening section, crucial for determining the dental class of the service member and ensuring that their dental needs align with the capabilities of the medical treatment facilities at the gaining location. This meticulous process, while voluntary, is critical, as failure to provide complete and accurate information can delay the screening process, affecting the assignment of orders and the overall transition for service and family members.
| Question | Answer |
|---|---|
| Form Name | Navmed 1300 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | navmed 1300 1 pdf fillable, navmed 1300 2, audiogram, navmed 1300 1 pdf |
MEDICAL, DENTAL AND EDUCATIONAL SUITABILITY SCREENING FOR SERVICE AND FAMILY
MEMBERS
Privacy Act Statement
Authority: 5 U.S.C. 301, Departmental Regulations; and E. O. 9397 (SSN).
Purpose: To identify medical, dental or educational conditions for the purpose of making a suitability recommendation for an overseas, remote duty, or operational assignment.
Routine uses: This form is completed by a military/civilian physician, nurse practioner, physician assistant, or independent duty corpsman. The medical treatment facility (MTF) Suitability Screening Coordinator will place the completed original form in the service or family member's MTF medical record and retain a copy for audit.
Disclosure: Voluntary; however, failure to provide this information may delay the screening process, result in orders held in abeyance until completion of screening or affect the amount of leave in transit.
Refer to BUMEDINST 1300.2A for implementing guidance. Complete one form for each service and family member screened.
SERVICE MEMBER NAME |
GRADE / RATE |
SSN |
FAMILY MEMBER NAME
FAMILY MEMBER PREFIX
SSN
NEXT DUTY STATION LOCATION & UNIT IDENTIFICATION CODE (UIC):
TYPE DUTY CLASSIFICATION CODE: (Navy enlisted only)
PART I
Medical Screening. Completed by the medical provider to identify special needs and determine if a service or family member is suitable for an overseas, remote duty, or operational assignment. Attach the completed Report of Medical History (DD
Yes No N/A |
ITEM |
1.All current health records (military and civilian) reviewed?
2.Physical examinations (aviation, submarine, radiation, asbestos, etc.) current and documented?
3.
4.Immunizations are
5.Reference audiogram documented on DD 2215?
6.Latest audiogram (DD 2216) reviewed?
7.HIV testing completed or drawn?
8.DNA testing completed and documented?
9.Are there pending consults or tests that have a bearing on assignment suitability?
10.Any past limited duty or medical board(s)? (document on DD
11.For all service members, annual preventive health assessment (PHA) current and documented?
12.For servicewomen:
a.Annual health assessment current and documented?
b.Pregnancy screening (verbal inquiry)?
|
|
c. If pregnant? (EDC: |
) |
13. |
For family members, U.S. Preventive Services Task Force screening test recommendations current and documented? |
||
|
|
|
|
|
14. |
If a Special Duty assignment, is there a condition, which by MANMED, chapter 15, section IV, is disqualifying? |
|
|
|
|
|
15.Are there any conditions requiring ongoing care in the following areas? (document on DD
a.Orthopedic conditions (e.g., chronic back, knee, joint pain or weakness)
b.Cardiovascular conditions (e.g., chest pain/angina, arrhythmia, valve disease, infarction)
c.Gynecologic conditions (e.g., chronic pelvic pain, abnormal PAP, breast mass)
d.Neurologic conditions (e.g., seizure, pinched nerve, migraine, neuropathy)
e.Respiratory conditions (e.g., asthma, RAD, chronic sinus, allergies)
f.Mental health or behavioral conditions (e.g., mood, adjustment/personality disorder, ADD/ADHD, anxiety, psychosis)
g.Recurrent or frequent medications not on the standard formulary (list on DD
h.Alcohol or substance abuse or dependence
i.Developmental concerns (e.g., motor, cognitive, communication, social/emotional, or adaptive development)
j.Specify other conditions or concerns:
16. For service/family members requiring medication in excess of 90 days: (if not applicable, check block and skip to #18)
a. Is the patient in the maintenance phase of treatment?
b.Should medication use cease, could the underlying condition become life threatening, pose a risk for dangerous or disruptive behavior or result in a limited duty, MEDEVAC, or early return situation?
c.Is the medical staff at the gaining MTF/operational platform capable of managing the medication manipulation(s) if the underlying condition exacerbates?
d.Has the service/family member registered with the TRICARE Mail Order Pharmacy program?
NAVMED 1300/1 (Rev.
Yes |
No N/A |
ITEM |
|
|
|
17. For service/family members with underlying medical conditions: (if not applicable, check block and skip to #18)
a. Is there a requirement for special medical supplies, adaptive equipment, assistive technology devices, special accommodations, etc.?
b.If exposed to a physically or emotionally demanding environment, could the underlying condition become life threatening, pose a risk for dangerous or disruptive behavior, or result in a limited duty or MEDEVAC situation?
c.Can the gaining MTF/operational platform provide the current required medical support?
d.Can the gaining MTF/operational platform provide required medical support (diagnostic and therapeutic) if the underlying condition is exacerbated?
e.Are there any chronic medical or mental health conditions requiring routine or continuing access to care or access to specialized medical care? (document on DD
f.If required, were potential environmental concerns and possible health effects communicated to each service and family member? (document on appropriate SF 600)
18.For infants and toddlers (birth through 2 years, inclusive) with a disability, is the child receiving or eligible to receive early intervention services as evidenced by an Individualized Family Service Plan (IFSP)?
19.For preschool and school children (ages 3 through 21, inclusive) with a disability, is the child receiving or eligible to receive special education and related services as evidenced by an Individualized Education Program (IEP) and DD 2792, Addendum B?
20.Specify other concerns:
IF ANY OF THE ABOVE SHADED BLOCKS ARE CHECKED, QUERY THE GAINING MEDICAL TREATMENT FACILITY OR MEDICAL DEPARTMENT SUPPORTING THE OVERSEAS, REMOTE DUTY OR OPERATIONAL LOCATION CONCERNING LOCAL CAPABILITIES TO PROVIDE REQUIRED SUPPORT. (Attach Reply)
Yes
No
IS THE SERVICE/FAMILY MEMBER SUITABLE FOR THE OVERSEAS, REMOTE DUTY OR OPERATIONAL ASSIGNMENT? (completed by an MTF medical screener only)
MTF Medical Screener (Signature) |
Date |
Civilian Medical Screener (Signature) |
Date |
Printed Name, Rank or Grade
Printed Name
MTF or Duty Station
Address
Telephone Number (include area/country code)
City, State, and ZIP Code
DSN Number
Telephone Number (include area/country code)
Telefax Number (include area/country code)
Telefax Number (include area/country code)
NAVMED 1300/1 (Rev.
PART II
SERVICE / FAMILY MEMBER NAME
GRADE / RATE / FAMILY MEMBER PREFIX
SSN
Dental Screening. Completed by a dental officer/privileged dentist prior to an overseas, remote duty, or operational assignment for the purpose of assessing and matching the dental needs of a service/family member to the support capabilities of the gaining medical treatment facility.
Yes No N/A |
ITEM |
1.All current dental records (military and civilian) reviewed?
2.All dental examinations are current? (If more than 180 days since last
3.Is a reexamination required by a Navy MTF if examined or treated at a
4. If service/family member is in Dental Class 3 or 4, can dental treatment or examination be completed before the transfer?
5.Is there a requirement for
6.Are there any chronic dental conditions requiring routine or continuing access to care or access to specialized dental care?
7.Specify other concerns:
8. Specify Dental Class: (required for service members) _____________
Dental Classifications: (Per DoDI 6025.19)
Normally considered worldwide deployable:
Class 1 - Patients with a current dental examination, who do not require dental treatment or
Class 2 - Patients with a current dental examination, who require
Normally not considered worldwide deployable:
Class 3 - Patients who require urgent or emergent dental treatment for oral conditions with a high potential to cause a dental emergency in the next 12 months.
Class 4 - Patients who require a dental examination either because: (1) No type 1 (comprehensive) or type 2 (annual or periodic oral) dental examination was completed by a dental officer/privileged dentist within the past 12 months; (2) A patient's dental record does not exist or;
(3) The dental record is not held by the responsible dental treatment facility or Medical Department activity.
IF ANY OF THE ABOVE SHADED BLOCKS ARE CHECKED, FORWARD A SUITABILITY INQUIRY TO THE GAINING MEDICAL TREATMENT FACILITY OR MEDICAL DEPARTMENT SUPPORTING THE OVERSEAS, REMOTE DUTY, OR OPERATIONAL LOCATION TO DETERMINE IF THE REQUIRED DENTAL SUPPORT IS AVAILABLE. (attach reply)
Yes
No
IS THE SERVICE/FAMILY MEMBER SUITABLE FOR THE OVERSEAS, REMOTE DUTY OR OPERATIONAL ASSIGNMENT? (completed by an MTF designated military dental screener only)
MTF Medical Screener (Signature) |
Date |
Civilian Medical Screener (Signature) |
Date |
Printed Name, Rank or Grade
Printed Name
DTF or Duty Station
Address
Telephone Number (include area/country code)
City, State, and ZIP Code
DSN Number
Telephone Number (include area/country code)
Telefax Number (include area/country code)
Telefax Number (include area/country code)
NAVMED 1300/1 (Rev.