
final supervision can be filled in in no time. Just open FormsPal PDF editor to complete the task quickly. In order to make our editor better and easier to use, we constantly design new features, with our users' suggestions in mind. Here is what you'd have to do to get going:
Step 1: First of all, open the pdf tool by clicking the "Get Form Button" in the top section of this site.
Step 2: With this online PDF tool, it's possible to do more than merely complete blanks. Express yourself and make your docs look perfect with customized textual content added in, or optimize the file's original content to perfection - all backed up by an ability to insert almost any graphics and sign it off.
When it comes to blank fields of this precise PDF, here's what you need to do:
1. To begin with, when filling out the final supervision, start with the part with the following fields:
2. Just after the last selection of blank fields is done, go on to enter the relevant details in these: Comments, Individual counseling skills, and Diagnoscidc skills Treatment.
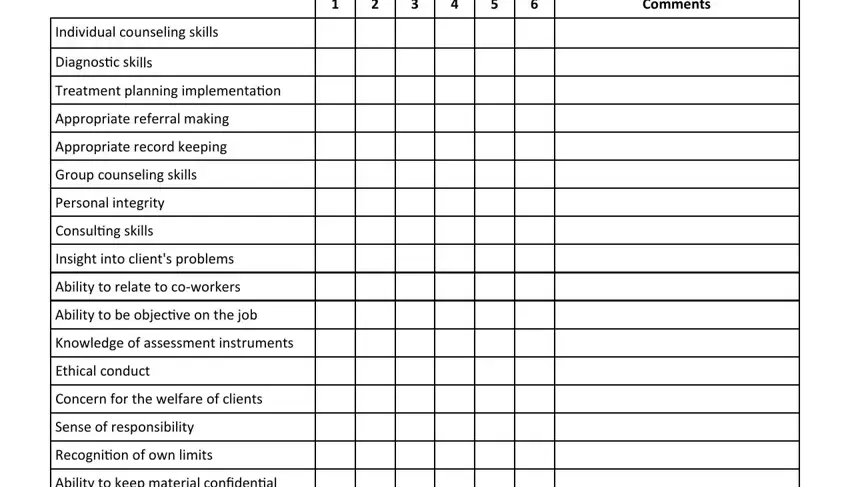
3. The next step will be simple - fill in every one of the form fields in Diagnoscidc skills Treatment, INITIAL Required, VI VERIFICATION To be completed, Supervisors Signature, Date, Acider complecidng this form, the NC Board of Licensed Clinical, and Page of to conclude the current step.
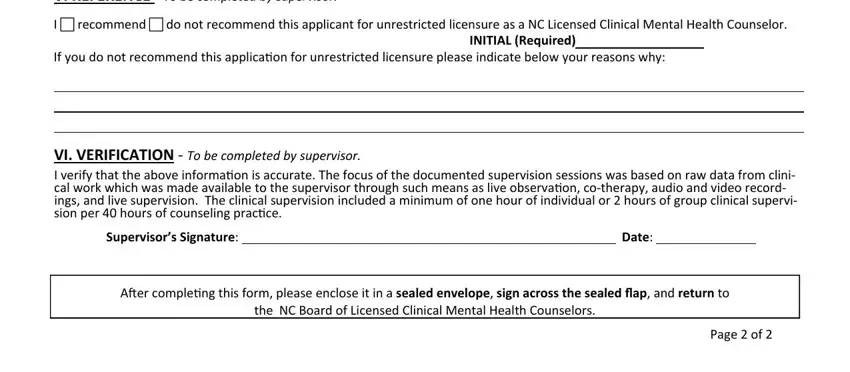
As to Page of and the NC Board of Licensed Clinical, be sure you do everything properly here. The two of these could be the most important ones in this PDF.
Step 3: Check all the details you have entered into the blank fields and click the "Done" button. After setting up afree trial account at FormsPal, you'll be able to download final supervision or send it via email immediately. The document will also be readily available in your personal account page with all of your changes. FormsPal ensures your information privacy by using a secure system that in no way saves or shares any type of personal data involved in the process. Be confident knowing your files are kept safe every time you use our services!