
nc form 22 can be filled in online effortlessly. Just open FormsPal PDF editing tool to complete the job quickly. Our editor is continually developing to present the best user experience attainable, and that is because of our dedication to continuous enhancement and listening closely to user comments. Here's what you will want to do to get started:
Step 1: First, open the tool by pressing the "Get Form Button" above on this site.
Step 2: This editor gives you the ability to modify your PDF document in various ways. Improve it with customized text, adjust what's originally in the PDF, and put in a signature - all when it's needed!
This form needs specific information; in order to guarantee consistency, don't hesitate to consider the subsequent tips:
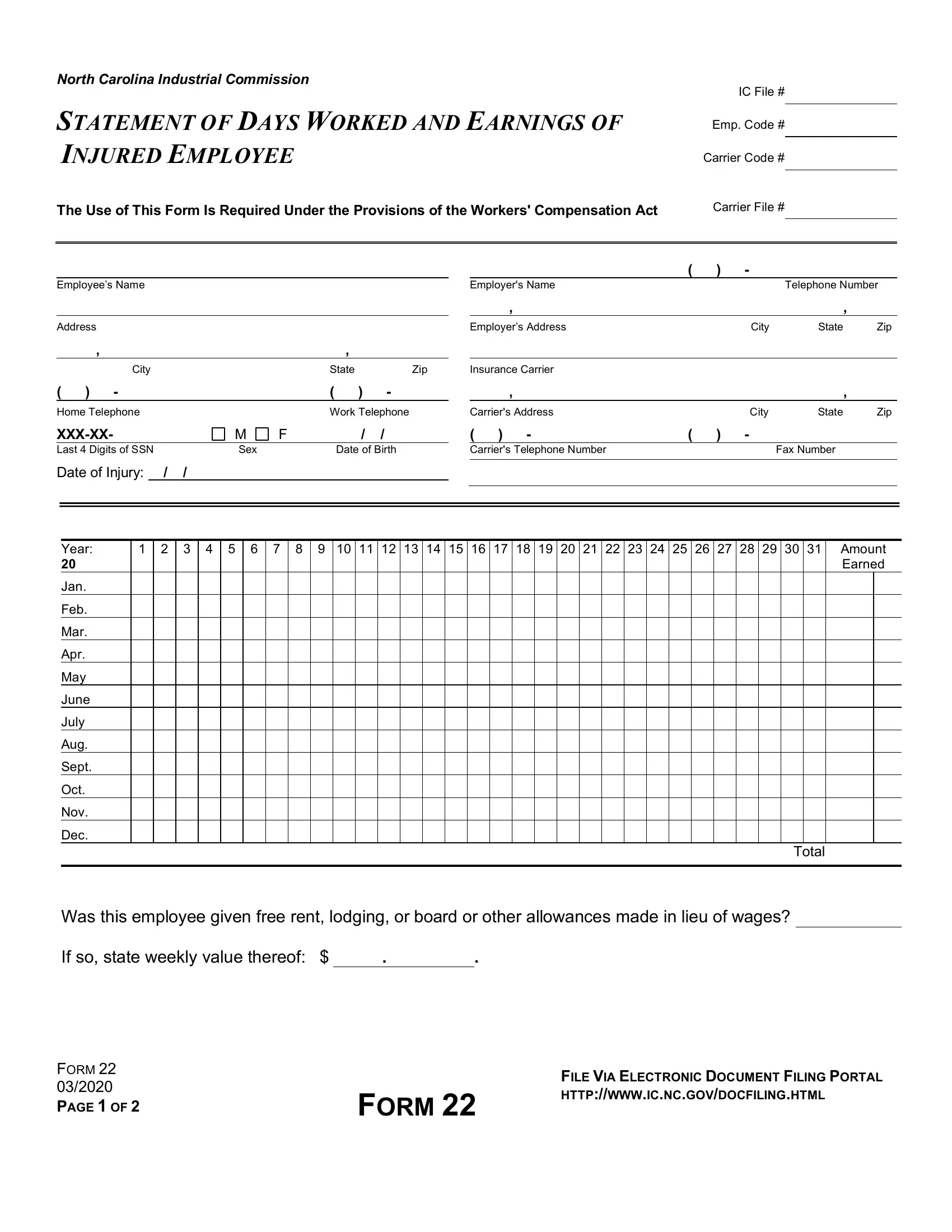
1. Complete your nc form 22 with a group of necessary blanks. Consider all of the important information and ensure there's nothing left out!
2. When the previous section is completed, go on to type in the applicable details in these: Year, Jan, Feb, Mar, Apr, May, June, July, Aug, Sept, Oct, Nov, Dec, Total, and Was this employee given free rent.
3. Completing The undersigned employer of who, Day, Name of Employee, Month, Year, while in the employment of the, Employer, Authorized Signature, Date Signed, To Employer Making a false, compensation benefits may result, and INSTRUCTIONS is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
As for Name of Employee and Month, be sure that you review things here. Those two are certainly the most important ones in the page.
Step 3: After you have looked once more at the information you filled in, click on "Done" to complete your FormsPal process. Find your nc form 22 once you sign up for a free trial. Readily view the pdf form inside your FormsPal account page, along with any edits and changes all kept! FormsPal guarantees your data confidentiality by having a secure method that never saves or shares any sort of personal information typed in. You can relax knowing your files are kept confidential any time you use our services!