


By using the online PDF tool by FormsPal, it is easy to fill out or alter Lightheadedness right here. To make our editor better and easier to work with, we continuously implement new features, taking into account suggestions from our users. If you're looking to begin, here is what it takes:
Step 1: First of all, access the tool by pressing the "Get Form Button" in the top section of this page.
Step 2: As you launch the editor, there'll be the form prepared to be filled in. Aside from filling out different blanks, you may as well do other sorts of actions with the PDF, such as writing any text, editing the initial text, adding images, placing your signature to the form, and much more.
When it comes to fields of this specific document, this is what you should know:
1. Begin completing the Lightheadedness with a selection of necessary blank fields. Gather all the necessary information and be sure not a single thing left out!
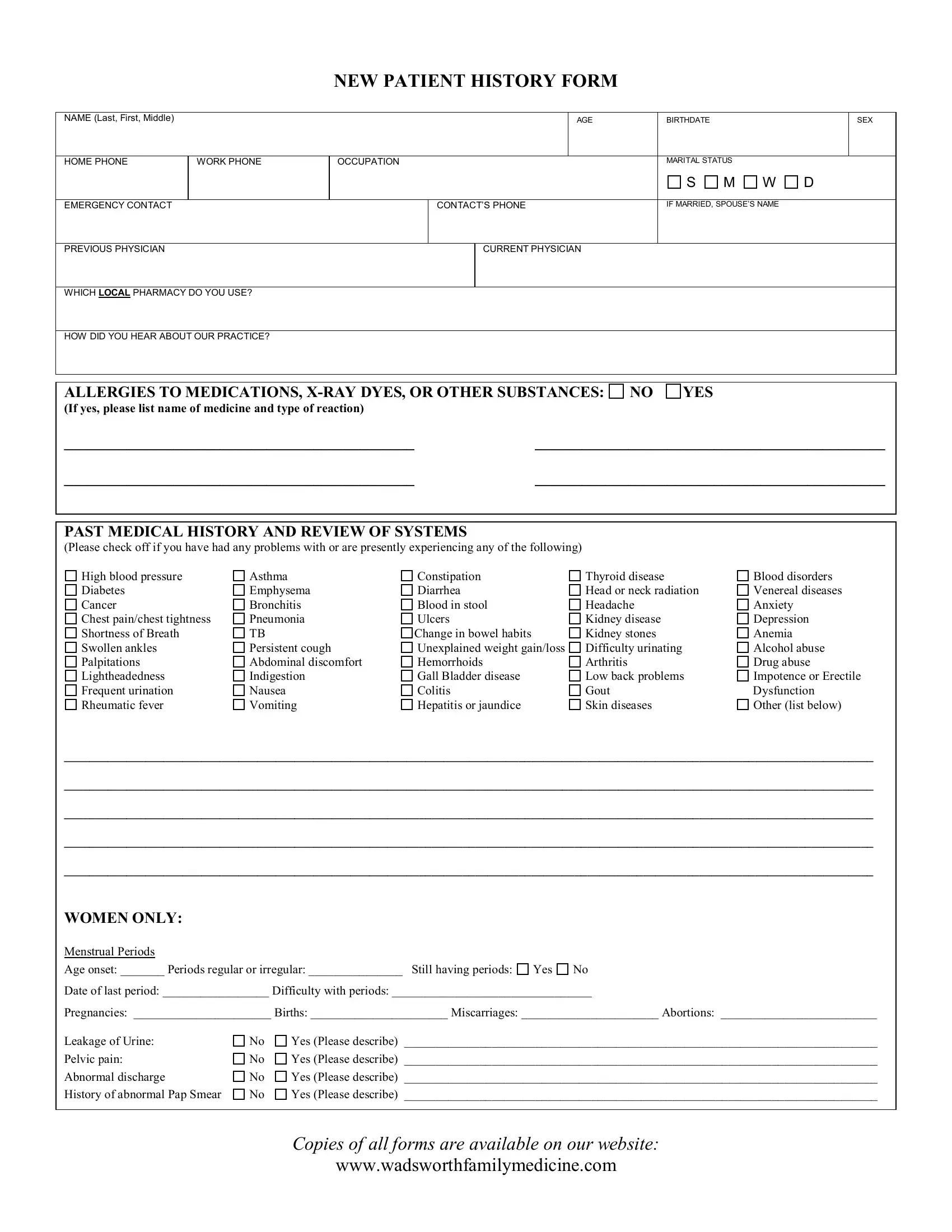
2. The third stage would be to complete all of the following fields: PAST MEDICAL HISTORY AND REVIEW OF, High blood pressure Diabetes, Asthma Emphysema Bronchitis, Constipation Diarrhea Blood in, Thyroid disease Head or neck, Blood disorders Venereal diseases, Other list below, and WOMEN ONLY Menstrual Periods.
3. In this step, have a look at WOMEN ONLY Menstrual Periods, Age onset Periods regular or, Yes, Date of last period Difficulty, Yes Please describe, Pelvic pain, Abnormal discharge, History of abnormal Pap Smear, Yes Please describe, Yes Please describe, Yes Please describe, Copies of all forms are available, and wwwwadsworthfamilymedicinecom. Each one of these need to be completed with highest awareness of detail.
4. It's time to complete the next form section! Here you'll get all these Review Date fields to fill out.
Be really careful while filling in Review Date and Review Date, because this is where many people make mistakes.
5. To finish your form, the last section includes a few additional blank fields. Entering OPERATIONS AND THEIR DATES, Tonsillectomy Appendectomy, Hernia Repair, Gallbladder, Other please list, HOSPITALIZATIONS Other than, FAMILY HISTORY Cancer describe, MOTHER, FATHER, and SIBLINGS is going to wrap up the process and you'll certainly be done in an instant!
Step 3: Before moving on, make certain that blanks are filled in right. Once you confirm that it's good, click “Done." Go for a free trial account at FormsPal and acquire instant access to Lightheadedness - download or modify inside your FormsPal cabinet. FormsPal guarantees your information confidentiality via a protected method that in no way records or shares any personal information used in the form. Be confident knowing your docs are kept confidential any time you use our service!