
The Confidential Patient Case History Form is a 2-page intake document that patients fill out before their first massage therapy appointment. It gives the therapist a complete picture of the patient's health so every session can be customized and safe.
What Information Does This Form Ask For?
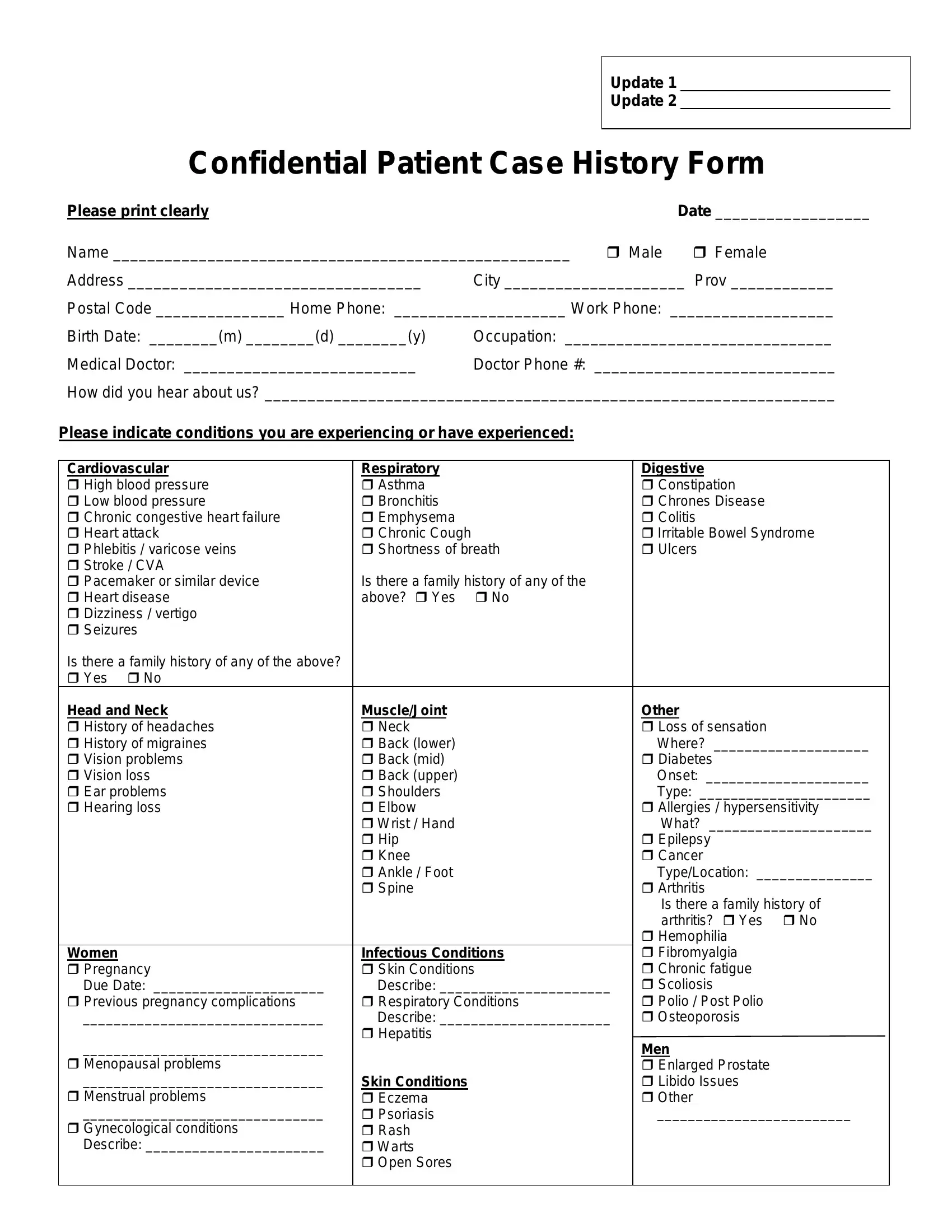
This form covers four main categories of patient information:
- Personal details: full name, address, date of birth, and contact information
- Medical history: current conditions, past surgeries, and current medications
- Family health history: hereditary conditions such as cardiovascular disease, cancer, or diabetes
- Lifestyle factors: physical activity levels, stress, and emotional well-being
How to Fill Out the Confidential Patient Case History Form Online
Follow these steps to complete the form using FormsPal's free PDF editor:
Step 1: Click the "Get Form" button at the top of this page to open the PDF editor.
Step 2: Enter your personal information in the fields provided, including your full name, date of birth, and contact details.
Step 3: Check all boxes that apply to your medical history. Include any conditions, surgeries, or medications relevant to your care.
Step 4: Complete the family history section by noting conditions such as heart disease, diabetes, or cancer that run in your family.
Step 5: Fill out the lifestyle section. Note your physical activity level, stress levels, and any areas of chronic pain or discomfort.
Step 6: Sign and date the form at the bottom. Download the completed PDF to share directly with your healthcare provider.
When Do You Need a Confidential Patient Case History Form?
Massage therapists and other complementary healthcare providers require this form before any treatment. The document protects both patient and therapist. It clearly establishes the scope and nature of the services provided. A thorough patient history helps therapists identify contraindications and adapt their approach for each individual.
You may also find these related forms useful: the Massage Intake Form, the Massage Health History Form, the Medical History Form, and the Patient Medication History Form.