
Working with PDF forms online is definitely simple with our PDF editor. You can fill out lottery claim form required for winnings here and try out many other functions available. FormsPal is dedicated to providing you the best possible experience with our editor by constantly releasing new functions and upgrades. Our editor is now a lot more useful thanks to the most recent updates! Now, editing documents is a lot easier and faster than ever before. Starting is simple! All you have to do is stick to these easy steps down below:
Step 1: Simply click on the "Get Form Button" at the top of this site to access our form editor. Here you will find all that is necessary to fill out your file.
Step 2: The editor will give you the ability to work with most PDF files in various ways. Transform it by including customized text, correct existing content, and place in a signature - all within a few clicks!
So as to finalize this PDF form, make certain you provide the right details in every single field:
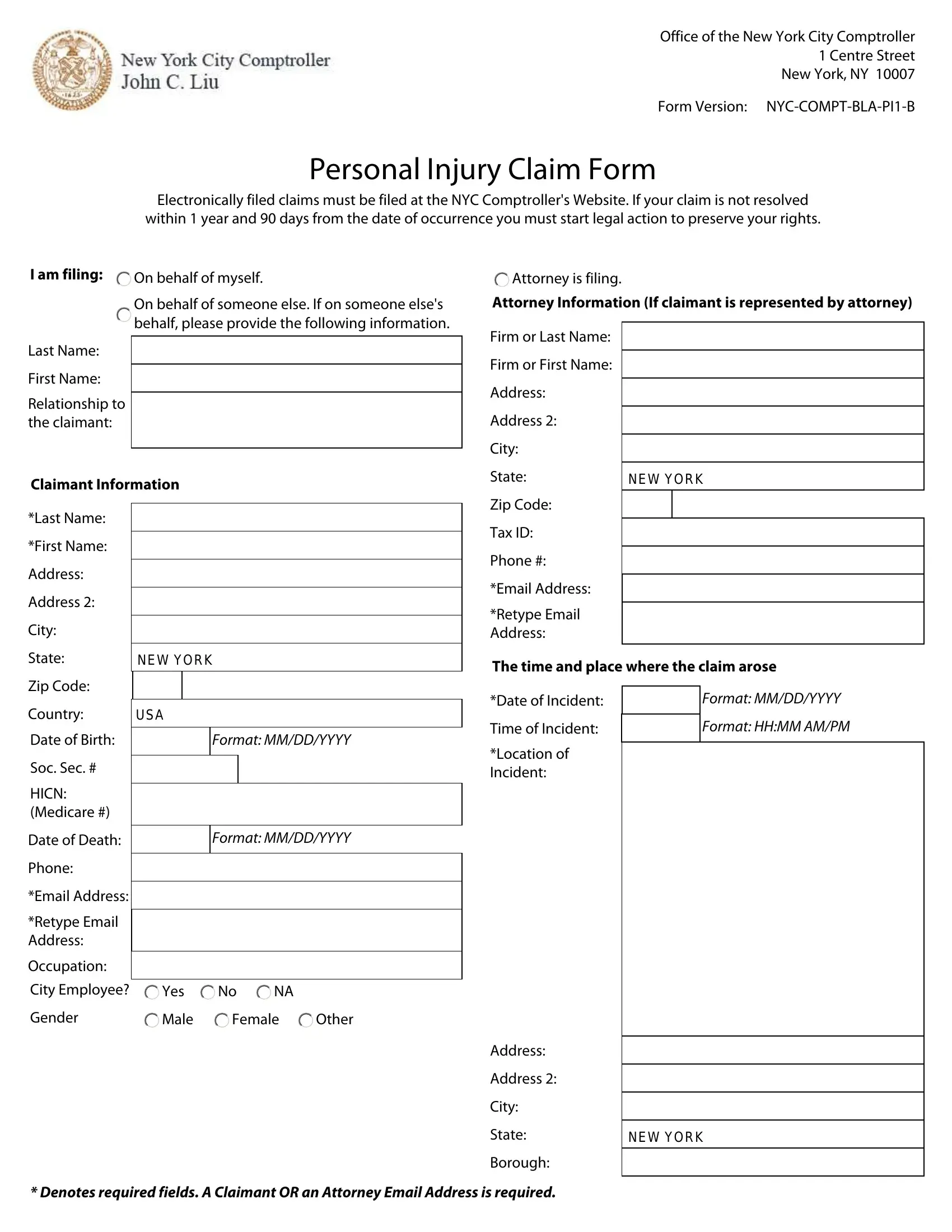
1. It is crucial to complete the lottery claim form required for winnings correctly, therefore be mindful when working with the segments containing all these blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Location of Incident, Format MMDDYYYY, Soc Sec, HICN Medicare, Date of Death, Phone, Email Address, Retype Email Address, Occupation, City Employee, Yes, Gender, Male, Female, and Other with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Completing Manner in which claim arose is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. Completing The items of damage or injuries is crucial in the next step - ensure to don't hurry and fill out every single blank!
Be really attentive when completing The items of damage or injuries and The items of damage or injuries, because this is where a lot of people make some mistakes.
5. The final step to submit this document is integral. You must fill out the mandatory fields, like Medical Information, Witness Information, st Treatment Date, Format MMDDYYYY, HospitalName, Address, Address, City, State, Zip Code, Date Treated in Emergency Room Was, Format MMDDYYYY, Yes, Employment Information If claiming, and Employers Name, prior to submitting. Neglecting to do so may give you a flawed and probably nonvalid document!
Step 3: Prior to addressing the next stage, check that all blanks were filled out as intended. When you establish that it is correct, click on “Done." Right after registering a7-day free trial account here, it will be possible to download lottery claim form required for winnings or send it via email promptly. The PDF form will also be readily available through your personal account page with your every single change. We don't share any information that you enter while completing forms at our website.