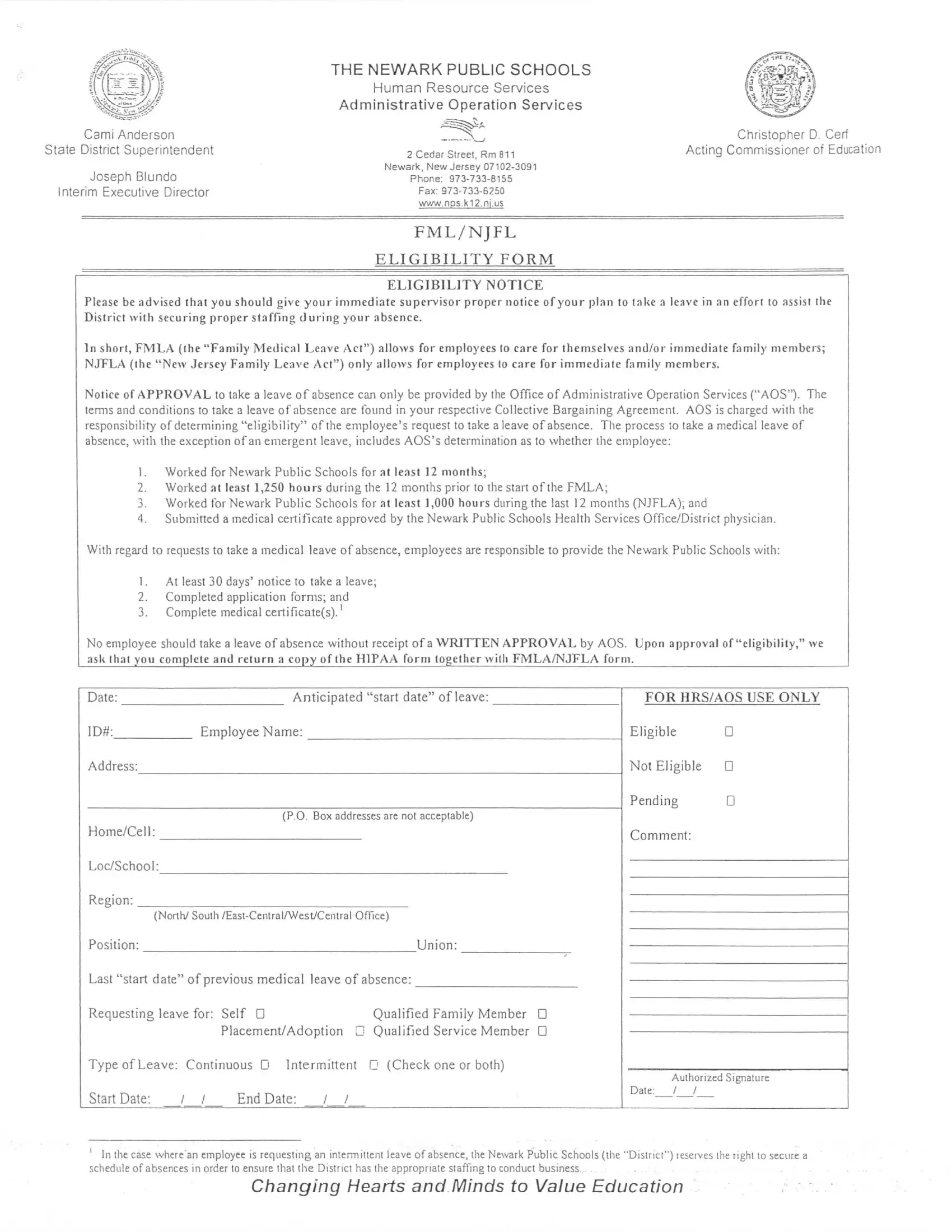
Navigating the intricacies of family and medical leave within the Newark Public Schools system can seem daunting at first glance. However, with the right information and understanding of the Newark Public Schools Lunch Application form, the process becomes clearer and more manageable. This comprehensive document not only outlines the procedures and requirements for applying for leave under the Family and Medical Leave Act (FMLA) and the New Jersey Family Leave Act (NJFLA) but also emphasizes the importance of communication between employees and their immediate supervisors during this process. It delineates eligibility criteria, such as the minimum months of service and hours worked, alongside the necessity of submitting a medical certificate. Moreover, the form underscores the district's commitment to support employees during their absence while ensuring minimal disruption to educational services. By providing detailed instructions on how to complete and submit the application, including necessary notices and medical certifications, the Newark Public Schools Lunch Application form serves as a critical resource for employees navigating the leave process, ultimately reflecting the district's broader mission to value and prioritize education even in the face of challenging circumstances.
| Question | Answer |
|---|---|
| Form Name | Newark Public Schools Lunch Application Form |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | newarkpublicschoolsfmlaforms, fmla new jersey application, how do i file for fmla in nj, emercency fmla in nj |