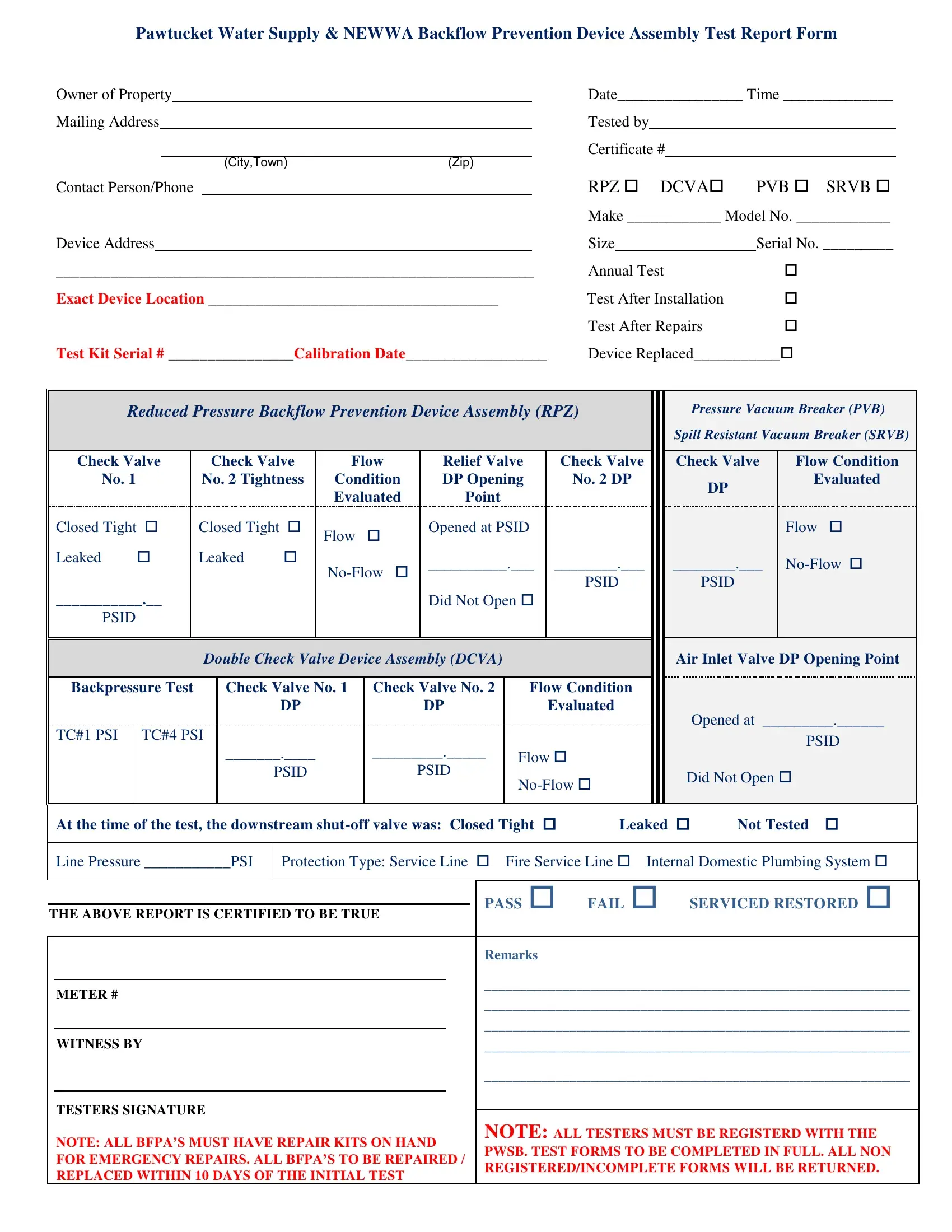
The Newwa Backflow Test Sheet form serves as a comprehensive document designed to record the testing and maintenance of backflow prevention device assemblies, ensuring the safety and integrity of water supply systems. This form is utilized primarily to document the condition and functionality of these devices, which are crucial for protecting water supplies from contamination due to backward flow. Property owners, alongside certified testers, fill out the form, noting details such as owner information, device specifics like make, model, and serial number, and the testing scenario, whether it's an annual test, a test after installation, repairs, or replacement. The form meticulously covers various types of devices, including Reduced Pressure Zone (RPZ) assemblies, Pressure Vacuum Breakers (PVB), Spill Resistant Vacuum Breakers (SRVB), and Double Check Valve Assemblies (DCVA), and records specific performance metrics like pressure and flow conditions, ensuring a detailed report on each device's operational status. With checkboxes to indicate the condition and outcome of each test and areas for remarks and technician signatures, the document emphasizes accountability and precision. It highlights the importance of backflow prevention in maintaining a clean and safe water supply by mandating regular inspection and maintenance, documented through this detailed form.
| Question | Answer |
|---|---|
| Form Name | NEWWA Backflow Test Sheet Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 73 |
| Avg. time to fill out | 14 min 55 sec |
| Other names | newwa backflow form, city of philadelphia backflow test form, asse test backflow forms pdf, newwa backflow test form |
Pawtucket Water Supply & NEWWA Backflow Prevention Device Assembly Test Report Form
Owner of Property |
|
|
Date________________ Time ______________ |
||||||||
Mailing Address |
|
|
|
|
Tested by |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Certificate # |
|
|
||
|
|
|
|
(City,Town) |
(Zip) |
|
|
|
|
|
|
Contact Person/Phone |
|
|
RPZ DCVA |
PVB SRVB |
|||||||
|
|
|
|
|
|
|
Make ____________ Model No. ____________ |
||||
Device Address |
|
|
|
Size |
|
Serial No. _________ |
|||||
_____________________________________________________________ |
Annual Test |
|
|||||||||
Exact Device Location _____________________________________ |
Test After Installation |
|
|||||||||
|
|
|
|
|
|
|
Test After Repairs |
|
|||
Test Kit Serial # ________________Calibration Date__________________ |
Device Replaced___________ |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Reduced Pressure Backflow Prevention Device Assembly (RPZ) |
|
Pressure Vacuum Breaker (PVB) |
||||||||||
|
|
|
|
|
|
|
|
|
Spill Resistant Vacuum Breaker (SRVB) |
|||
Check Valve |
Check Valve |
Flow |
Relief Valve |
Check Valve |
Check Valve |
Flow Condition |
||||||
No. 1 |
|
No. 2 Tightness |
Condition |
DP Opening |
No. 2 DP |
|
DP |
Evaluated |
||||
|
|
|
|
Evaluated |
Point |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
Closed Tight |
Closed Tight |
Flow |
|
Opened at PSID |
|
|
|
Flow |
|
|||
Leaked |
|
Leaked |
|
__________.___ ________.___ |
________.___ |
|||||||
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
PSID |
|
PSID |
|
|
___________.__ |
|
|
|
|
Did Not Open |
|
|
|
|
|
||
PSID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Double Check Valve Device Assembly (DCVA) |
|
|
Air Inlet Valve DP Opening Point |
|||||||
Backpressure Test |
Check Valve No. 1 |
Check Valve No. 2 |
Flow Condition |
|
|
|
|
|||||
|
|
|
DP |
|
|
DP |
|
Evaluated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Opened at _________.______ |
||
TC#1 PSI |
TC#4 PSI |
|
|
|
|
|
|
|
|
PSID |
||
|
|
_______.____ |
|
_________._____ |
Flow |
|
|
|||||
|
|
|
|
|
|
|
||||||
|
|
|
PSID |
|
|
PSID |
Did Not Open |
|
||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||
At the time of the test, the downstream |
Leaked |
Not Tested |
|
|||||||||
Line Pressure ___________PSI |
Protection Type: Service Line |
Fire Service Line Internal Domestic Plumbing System |
||||||||||
THE ABOVE REPORT IS CERTIFIED TO BE TRUE |
PASS FAIL SERVICED RESTORED |
||
|
|||
|
|
|
Remarks |
|
|
|
____________________________________________________________ |
|
METER # |
||
|
____________________________________________________________ |
||
|
|
|
|
|
|
|
____________________________________________________________ |
|
WITNESS BY |
||
|
____________________________________________________________ |
||
|
|
|
____________________________________________________________ |
|
|
|
|
|
TESTERS SIGNATURE |
|
|
|
NOTE: ALL BFPA’S MUST HAVE REPAIR KITS ON HAND |
NOTE: ALL TESTERS MUST BE REGISTERD WITH THE |
|
|
PWSB. TEST FORMS TO BE COMPLETED IN FULL. ALL NON |
||
|
FOR EMERGENCY REPAIRS. ALL BFPA’S TO BE REPAIRED / |
||
|
REGISTERED/INCOMPLETE FORMS WILL BE RETURNED. |
||
|
REPLACED WITHIN 10 DAYS OF THE INITIAL TEST |
||
|
|
||