

You'll be able to prepare nexxus form sample instantly by using our PDFinity® online PDF tool. To retain our tool on the leading edge of efficiency, we work to put into action user-driven features and enhancements regularly. We're at all times pleased to receive feedback - join us in revampimg PDF editing. It just takes several easy steps:
Step 1: Click the "Get Form" button in the top area of this webpage to access our editor.
Step 2: Using this advanced PDF editing tool, you could do more than simply complete blanks. Edit away and make your documents look sublime with customized textual content added in, or fine-tune the file's original input to excellence - all that supported by an ability to insert almost any photos and sign it off.
To be able to fill out this PDF document, be sure you type in the required details in every blank field:
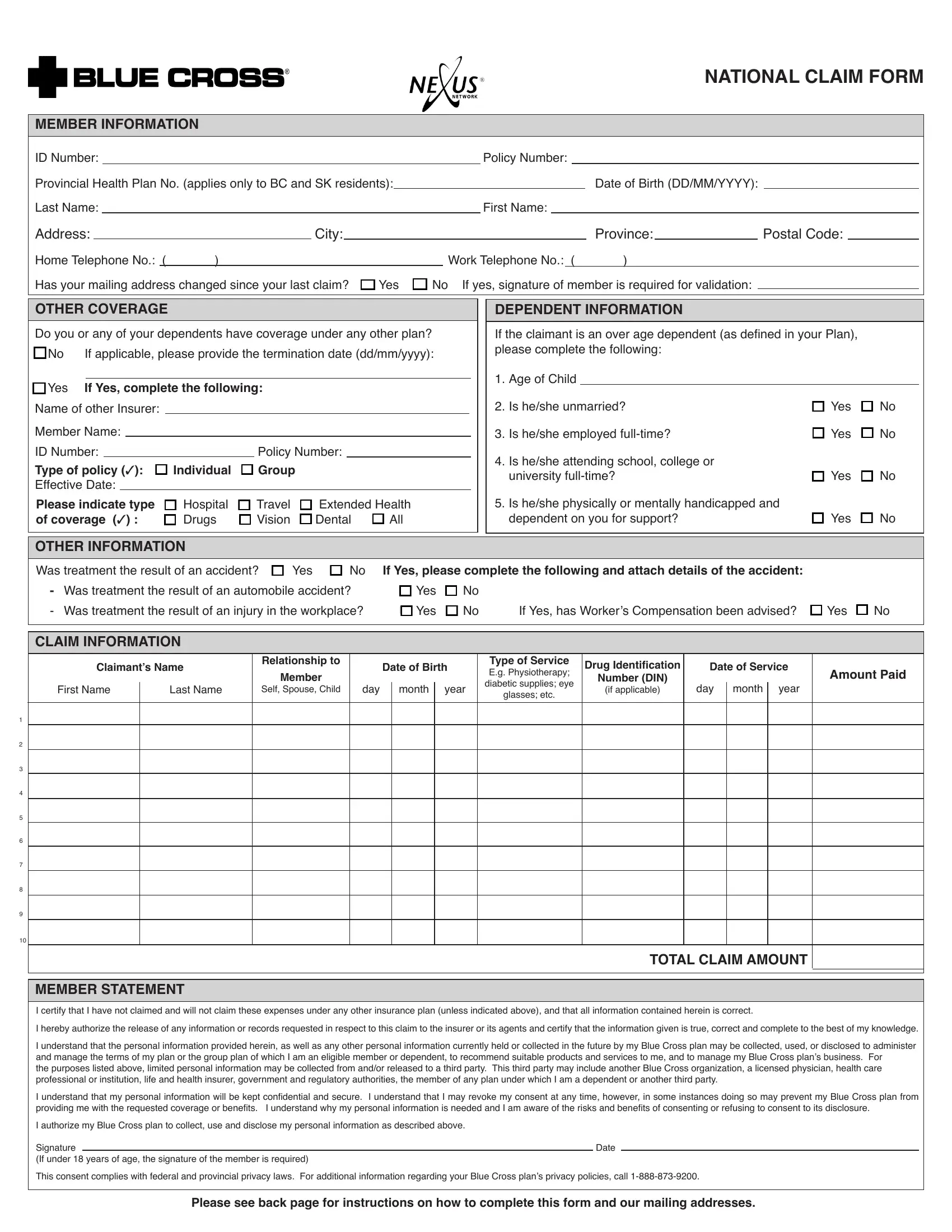
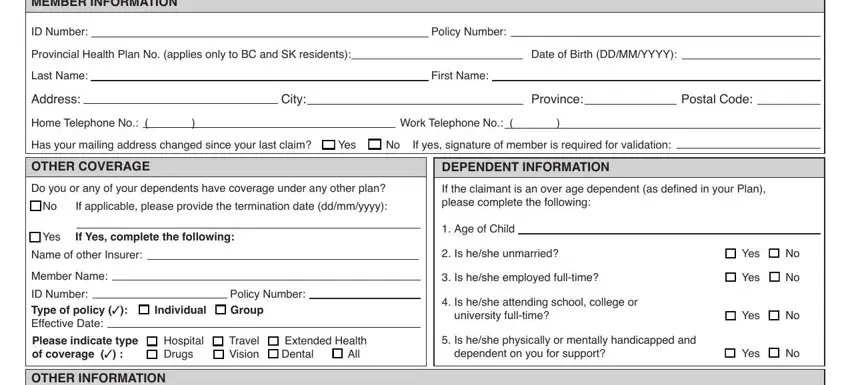
1. Before anything else, once filling in the nexxus form sample, start in the area containing subsequent fields:
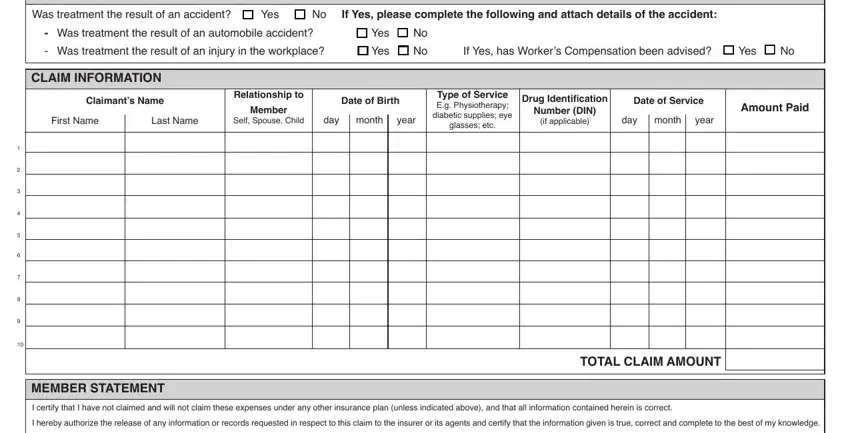
2. Your next stage would be to submit these particular blanks: q Yes If Yes complete the, Was treatment the result of an, q Yes q No q Yes q No, Drug Identiication, Relationship to, Date of Service, Date of Birth, First Name, Last Name, Member, Self Spouse Child, day month, year, If Yes has Workers Compensation, and Type of Service Eg Physiotherapy.
People often make some mistakes when filling out If Yes has Workers Compensation in this section. You should definitely reread what you enter right here.
3. This subsequent step is pretty straightforward, MEMBER STATEMENT I certify that I, Date, and Please see back page for - every one of these blanks has to be filled out here.

Step 3: Right after you have glanced through the details in the blanks, click "Done" to finalize your form at FormsPal. Right after getting a7-day free trial account with us, you'll be able to download nexxus form sample or send it through email right off. The PDF will also be at your disposal through your personal cabinet with all of your modifications. When using FormsPal, you're able to fill out documents without worrying about personal information incidents or records being distributed. Our secure software ensures that your private data is kept safely.