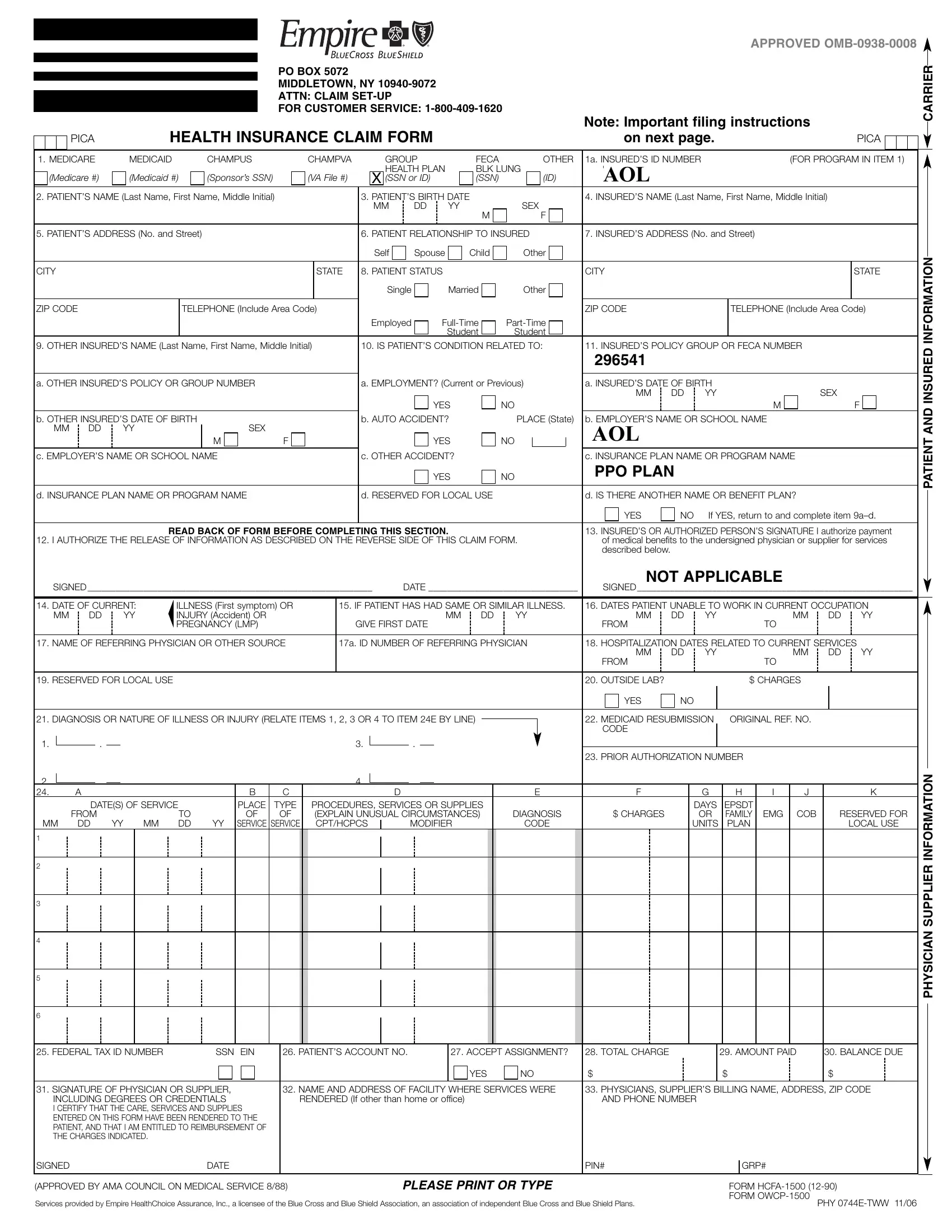
Filing a health insurance claim with Empire Blue Cross requires thorough attention to detail, especially when using the Empire Blue Cross Claim form. This form serves as a crucial document for individuals seeking reimbursement or direct payment for healthcare services from providers outside the Empire Blue Cross network. It encapsulates various sections, including patient and insured information, physician or supplier details, and comprehensive instructions to ensure accurate and complete submission. Whether the healthcare services arise from routine visits, emergency treatment, or are related to employment, auto accidents, or another incident, every aspect must be meticulously documented. The form uniquely identifies each claim through details such as Medicare, Medicaid, or other insurance information, alongside personal identifiers like the insured's ID and patient's relationship to the insured. Moreover, it factors in the complexities of healthcare services, addressing situations involving other insured policies, employment-related conditions, and specifics about the healthcare provider. To facilitate the processing of claims, it mandates the attachment of original itemized bills or the completion of sections dedicated to the services provided. Empire Blue Cross emphasizes the need for the patient’s or their legal guardian's authorization, both for the release of pertinent medical information and for the understanding of the financial aspects, such as charges, payments, and balances due. Additionally, it stipulates clear guidelines aimed at preventing fraudulent claims, underscoring the legal implications of submitting false information. Through this form, Empire Blue Cross outlines a structured pathway for members to claim their benefits, ensuring transparency and efficiency in handling healthcare expenses.
| Question | Answer |
|---|---|
| Form Name | Empire Blue Cross Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | phy tww blue template, empire hcfa blue shield, tww claim blue cross, empire bcbs claim form |
APPROVED
|
|
PO BOX 5072 |
|
|
|
|
|
|
|
MIDDLETOWN, NY |
|
|
|
ATTN: CLAIM |
|
|
|
FOR CUSTOMER SERVICE: |
Note: Important filing instructions |
|
|
||
|
|
|
|
PICA |
HEALTH INSURANCE CLAIM FORM |
on next page. |
|
CARRIER
PICA
1. MEDICARE |
|
|
MEDICAID |
|
|
CHAMPUS |
|
|
CHAMPVA |
|
|
|
GROUP |
|
|
|
FECA |
|
|
|
OTHER |
1a. INSURED’S ID NUMBER |
|
|
|
|
|
|
(FOR PROGRAM IN ITEM 1) |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEALTH PLAN |
|
|
BLK LUNG |
|
|
TWWAOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
(Medicare #) |
|
|
(Medicaid #) |
(Sponsor’s SSN) |
|
|
(VA File #) |
|
|
X (SSN or ID) |
|
|
|
(SSN) |
|
|
|
(ID) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. PATIENT’S NAME (Last Name, First Name, Middle Initial) |
|
|
|
|
3. PATIENT’S BIRTH DATE |
|
|
|
|
|
|
|
|
|
|
4. INSURED’S NAME (Last Name, First Name, Middle Initial) |
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
|
DD |
|
|
YY |
|
|
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
5. PATIENT’S ADDRESS (No. and Street) |
|
|
|
|
|
|
|
|
|
6. PATIENT RELATIONSHIP TO INSURED |
7. INSURED’S ADDRESS (No. and Street) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
Child |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|
8. PATIENT STATUS |
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATE |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single |
|
|
Married |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
ZIP CODE |
|
|
|
|
|
TELEPHONE (Include Area Code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ZIP CODE |
|
|
|
|
|
|
TELEPHONE (Include Area Code) |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Student |
Student |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
9. OTHER INSURED’S NAME (Last Name, First Name, Middle Initial) |
|
10. IS PATIENT’S CONDITION RELATED TO: |
11. INSURED’S POLICY GROUP OR FECA NUMBER |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
296541 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
a. OTHER INSURED’S POLICY OR GROUP NUMBER |
|
|
|
|
|
|
a. EMPLOYMENT? (Current or Previous) |
a. INSURED’S DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
DD |
YY |
|
|
|
|
|
|
|
SEX |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
F |
||||||||
b. OTHER INSURED’S DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
b. AUTO ACCIDENT? |
|
|
|
PLACE (State) |
b. EMPLOYER’S NAME OR SCHOOL NAME |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
MM |
DD |
|
YY |
|
|
M |
SEX |
|
F |
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
NO |
|
|
|
|
|
|
|
AOLTIME WARNER, INC. |
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. EMPLOYER’S NAME OR SCHOOL NAME |
|
|
|
|
|
|
|
|
c. OTHER ACCIDENT? |
|
|
|
|
|
|
|
|
|
|
c. INSURANCE PLAN NAME OR PROGRAM NAME |
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
NO |
|
PPO PLAN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
d. INSURANCE PLAN NAME OR PROGRAM NAME |
|
|
|
|
|
|
d. RESERVED FOR LOCAL USE |
|
|
|
|
|
|
|
d. IS THERE ANOTHER NAME OR BENEFIT PLAN? |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
If YES, return to and complete item |
|||||||||||||||
|
|
|
|
|
|
|
READ BACK OF FORM BEFORE COMPLETING THIS SECTION. |
|
|
|
|
|
|
|
|
|
|
13. INSURED’S OR AUTHORIZED PERSON’S SIGNATURE I authorize payment |
|||||||||||||||||||||||||||||||||||||||
12. I AUTHORIZE THE RELEASE OF INFORMATION AS DESCRIBED ON THE REVERSE SIDE OF THIS CLAIM FORM. |
|
of medical benefits to the undersigned physician or supplier for services |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
described below. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOT APPLICABLE |
|
|
|
|
|
|
|||||||||||
SIGNED _____________________________________________________________ |
DATE ________________________________ |
|
SIGNED ___________________________________________________________ |
||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
14. DATE OF CURRENT: |
ILLNESS (First symptom) OR |
|
|
15. IF PATIENT HAS HAD SAME OR SIMILAR ILLNESS. |
16. DATES PATIENT UNABLE TO WORK IN CURRENT OCCUPATION |
||||||||||||||||||||||||||||||||||||||||||||||||||||
MM |
DD |
|
|
YY |
INJURY (Accident) OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
DD |
YY |
|
|
MM |
DD |
YY |
|
|
|
|
|
|
MM |
|
DD |
|
YY |
||||||||||||||||||||
|
|
|
|
|
|
|
|
PREGNANCY (LMP) |
|
|
|
|
|
GIVE FIRST DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
TO |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
17. NAME OF REFERRING PHYSICIAN OR OTHER SOURCE |
|
|
17a. ID NUMBER OF REFERRING PHYSICIAN |
18. HOSPITALIZATION DATES RELATED TO CURRENT SERVICES |
|||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MM |
DD |
YY |
|
|
|
|
|
|
MM |
|
DD |
|
YY |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
TO |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
19. RESERVED FOR LOCAL USE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. OUTSIDE LAB? |
|
|
|
|
|
|
|
$ CHARGES |
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
21. DIAGNOSIS OR NATURE OF ILLNESS OR INJURY (RELATE ITEMS 1, 2, 3 OR 4 TO ITEM 24E BY LINE) |
|
|
|
|
|
|
|
|
22. MEDICAID RESUBMISSION |
|
|
ORIGINAL REF. NO. |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23. PRIOR AUTHORIZATION NUMBER |
|
|
|
|
|
|
|
||||||||||||
2. |
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
24. |
|
A |
|
|
|
|
|
|
|
B |
|
|
C |
|
|
|
|
|
|
|
D |
|
|
|
|
|
|
|
|
E |
|
|
F |
|
|
G |
|
|
H |
I |
J |
|
|
|
|
K |
|||||||||||
|
|
DATE(S) OF SERVICE |
|
PLACE |
|
TYPE |
PROCEDURES, SERVICES OR SUPPLIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAYS |
|
EPSDT |
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
FROM |
|
|
|
|
TO |
|
OF |
|
OF |
|
(EXPLAIN UNUSUAL CIRCUMSTANCES) |
|
DIAGNOSIS |
|
|
$ CHARGES |
|
|
OR |
|
FAMILY |
EMG |
COB |
|
|
RESERVED FOR |
|||||||||||||||||||||||||||||
MM |
DD |
YY |
|
MM |
DD |
YY |
SERVICE |
SERVICE |
|
CPT/HCPCS |
|
|
MODIFIER |
|
|
|
CODE |
|
|
|
|
|
UNITS |
|
PLAN |
|
|
|
|
|
LOCAL USE |
||||||||||||||||||||||||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
25. FEDERAL TAX ID NUMBER |
|
|
SSN |
EIN |
|
26. PATIENT’S ACCOUNT NO. |
|
|
27. ACCEPT ASSIGNMENT? |
28. TOTAL CHARGE |
|
|
|
|
29. AMOUNT PAID |
|
30. BALANCE DUE |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
$ |
|
|
|
|
|
|
$ |
|
|
|
|
|
|
$ |
|
|
|||||||||||
31. SIGNATURE OF PHYSICIAN OR SUPPLIER, |
|
|
|
32. NAME AND ADDRESS OF FACILITY WHERE SERVICES WERE |
33. PHYSICIANS, SUPPLIER’S BILLING NAME, ADDRESS, ZIP CODE |
||||||||||||||||||||||||||||||||||||||||||||||||||||
INCLUDING DEGREES OR CREDENTIALS |
|
|
|
RENDERED (If other than home or office) |
|
|
|
|
|
|
|
|
|
|
|
AND PHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
I CERTIFY THAT THE CARE, SERVICES AND SUPPLIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
ENTERED ON THIS FORM HAVE BEEN RENDERED TO THE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
PATIENT, AND THAT I AM ENTITLED TO REIMBURSEMENT OF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
THE CHARGES INDICATED. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
SIGNED |
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PIN# |
|
|
|
|
|
|
|
GRP# |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
(APPROVED BY AMA COUNCIL ON MEDICAL SERVICE 8/88) |
|
|
|
|
|
|
|
PLEASE PRINT OR TYPE |
|
|
|
|
|
|
|
|
|
|
FORM |
|
|
||||||||||||||||||||||||||||||||||||
Services provided by Empire HealthChoice Assurance, Inc., a licensee of the Blue Cross and Blue Shield Association, an association of independent Blue Cross and Blue Shield Plans. |
|
|
|
|
|
|
FORM |
PHY |
|||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
PATIENT AND INSURED INFORMATION
PHYSICIAN SUPPLIER INFORMATION