
Using PDF forms online is definitely a piece of cake using our PDF tool. You can fill out nf form 3 here effortlessly. To maintain our tool on the cutting edge of convenience, we strive to put into operation user-driven features and enhancements regularly. We are routinely looking for feedback - play a vital part in revampimg PDF editing. To get the ball rolling, take these easy steps:
Step 1: Simply press the "Get Form Button" in the top section of this site to see our pdf file editor. Here you will find everything that is needed to fill out your file.
Step 2: With our state-of-the-art PDF editing tool, it is easy to do more than just complete blanks. Edit away and make your forms seem sublime with customized text put in, or adjust the original input to perfection - all comes along with an ability to add just about any images and sign the document off.
With regards to the fields of this particular document, this is what you should know:
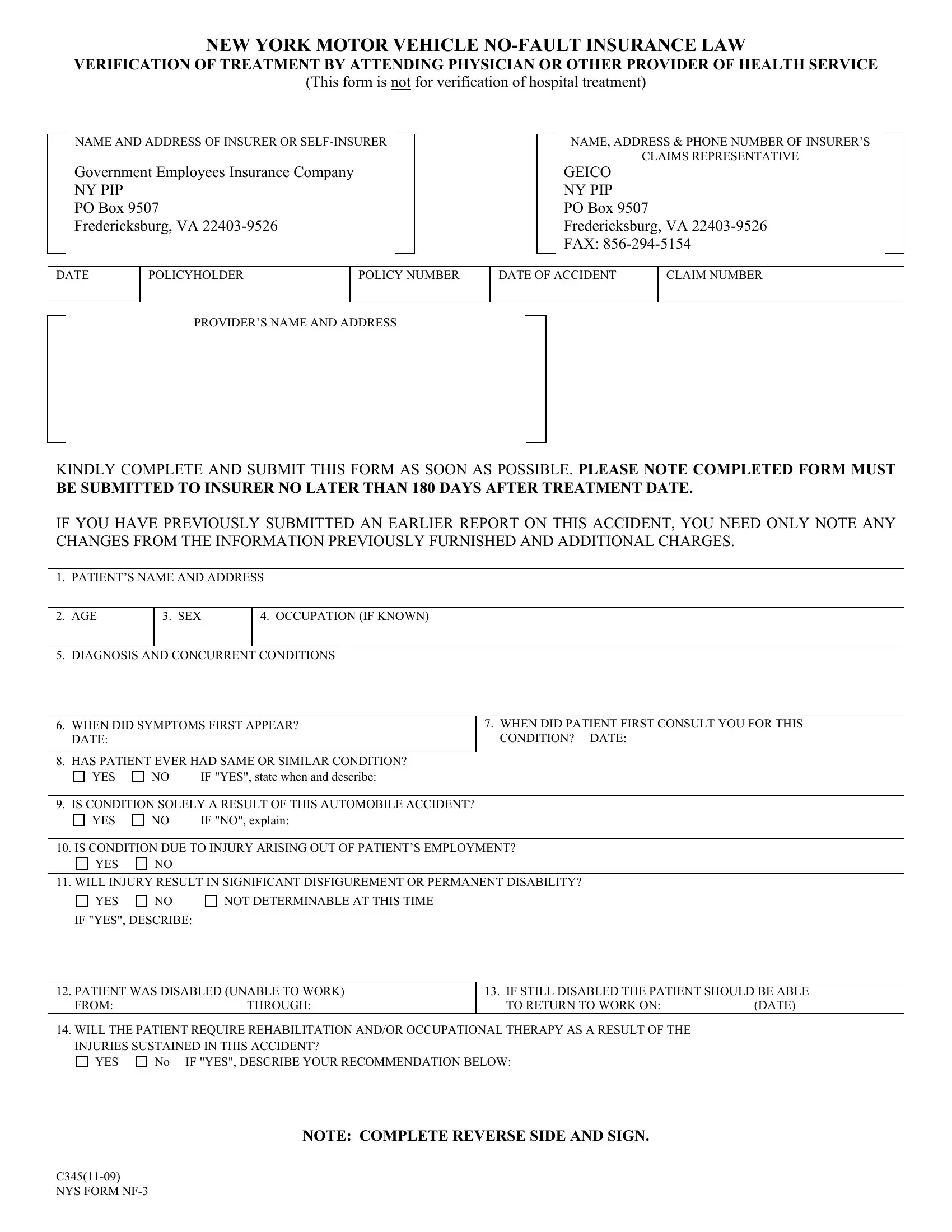
1. Complete your nf form 3 with a selection of essential fields. Gather all the necessary information and be sure not a single thing overlooked!
2. Once your current task is complete, take the next step – fill out all of these fields - IS CONDITION SOLELY A RESULT OF, NO IF NO explain, YES, IS CONDITION DUE TO INJURY, YES, WILL INJURY RESULT IN SIGNIFICANT, YES, NOT DETERMINABLE AT THIS TIME, IF YES DESCRIBE, PATIENT WAS DISABLED UNABLE TO, No IF YES DESCRIBE YOUR, YES, IF STILL DISABLED THE PATIENT, C NYS FORM NF, and NOTE COMPLETE REVERSE SIDE AND SIGN with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. The next segment is pretty uncomplicated, DATE OF SERVICE, PLACE OF SERVICE, INCLUDING ZIP CODE, DESCRIPTION OF TREATMENT OR, HEALTH SERVICE RENDERED, FEE SCHEDULE, TREATMENT CODE, CHARGES, TOTAL CHARGES TO DATE, IF TREATING PROVIDER IS DIFFERENT, TREATING PROVIDERS, NAME, TITLE, LICENSE OR, and CERTIFICATION NUMBER - every one of these empty fields needs to be filled out here.
Regarding LICENSE OR and DATE OF SERVICE, ensure that you don't make any errors in this section. The two of these could be the most significant ones in the form.
4. This next section requires some additional information. Ensure you complete all the necessary fields - OPTIONAL ASSIGNMENT OF NOFAULT, IRSTIN IDENTIFICATION NO, PROVIDERS SIGNATURE, WCB RATING CODE, C NYS FORM NF, and IF NONE SPECIALTY - to proceed further in your process!
Step 3: Once you have glanced through the details you given, click on "Done" to conclude your FormsPal process. Sign up with FormsPal now and instantly gain access to nf form 3, ready for download. All changes you make are preserved , which enables you to modify the form at a later point anytime. Here at FormsPal, we do our utmost to make sure that your details are stored private.