The objective behind our PDF editor was to ensure it is as convenient as it can be. You will find the general procedure of completing nj family care application nj easy in case you stick to the next actions.
Step 1: At first, click the orange "Get form now" button.
Step 2: You are now on the form editing page. You can edit, add text, highlight selected words or phrases, put crosses or checks, and put images.
Feel free to type in the next information to complete the nj family care application nj PDF:
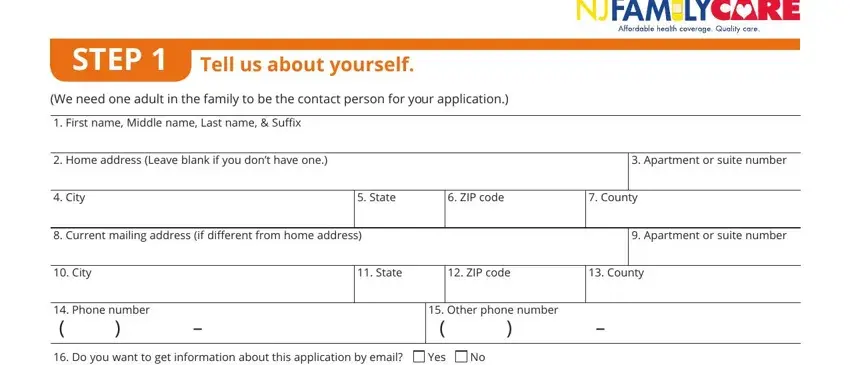
Enter the appropriate information in the area STEP, Tell us about yourself, We need one adult in the family to, First name Middle name Last name, Home address Leave blank if you, Apartment or suite number, City, State, ZIP code, County, Current mailing address if, Apartment or suite number, City, State, and ZIP code.
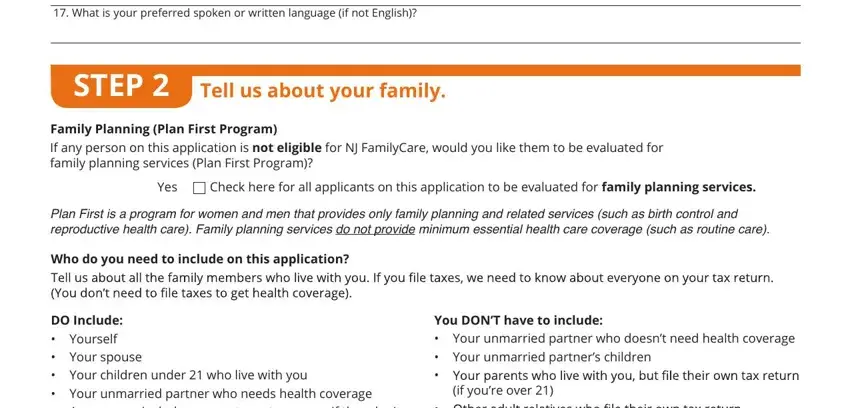
Describe the most important details the What is your preferred spoken or, STEP, Tell us about your family, Family Planning Plan First Program, If any person on this application, Yes Check here for all applicants, Plan First is a program for women, Who do you need to include on this, DO Include Yourself cid Your, You DONT have to include cid cid, Your unmarried partner who doesnt, if youre over, and cid segment.
Take the time to place the rights and obligations of the sides inside the with you, First name Middle name Last name, Relationship to you, SELF, Date of birth mmddyyyy, Sex, Male, Female, dettimdA yllufwaL toN eelysA, Social Security number SSN, We need this if you want health, Check this box if you plan to file, Will you file jointly with your, Yes No, and If yes name of spouse box.
Fill in the form by looking at all of these areas: Are you pregnant, Yes, No a, If yes, how many babies are expected durin, g this pregnancy, Due Date, Do you need health coverage, Even if you have insurance there, YES If yes answer all the, NO If no SKIP to the income, Do you have a physical mental or, chores etc or live in a medical, Yes, and Do you want help paying for.
Step 3: As soon as you've clicked the Done button, your document is going to be ready for export to every device or email you specify.
Step 4: Produce a copy of each separate file. It can save you some time and enable you to prevent concerns as time goes on. By the way, the information you have will not be shared or checked by us.
