

Using PDF files online is a breeze with our PDF tool. You can fill out florida medical nursing form here and use a number of other options we offer. The tool is consistently improved by us, acquiring additional functions and turning out to be better. Here's what you'll need to do to get going:
Step 1: Access the PDF form inside our editor by pressing the "Get Form Button" above on this page.
Step 2: As you start the tool, you will find the form all set to be filled out. Besides filling out different blank fields, you could also perform some other actions with the form, particularly putting on any words, changing the initial text, adding illustrations or photos, affixing your signature to the PDF, and more.
If you want to complete this document, be sure to enter the information you need in every single area:
1. Whenever submitting the florida medical nursing form, ensure to incorporate all needed blanks in its corresponding section. This will help expedite the process, which allows your information to be handled efficiently and appropriately.
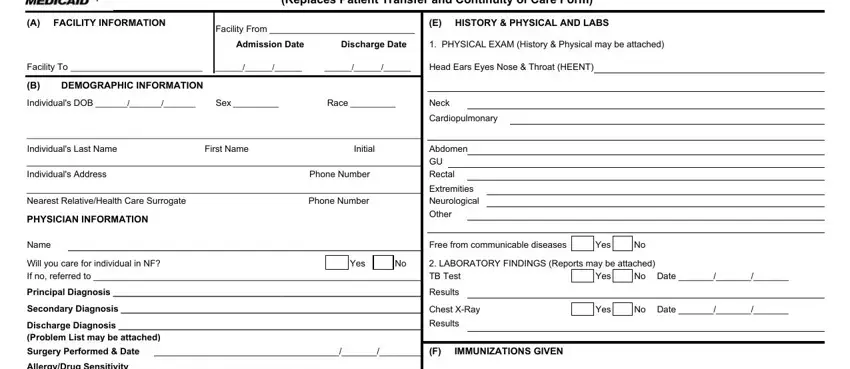
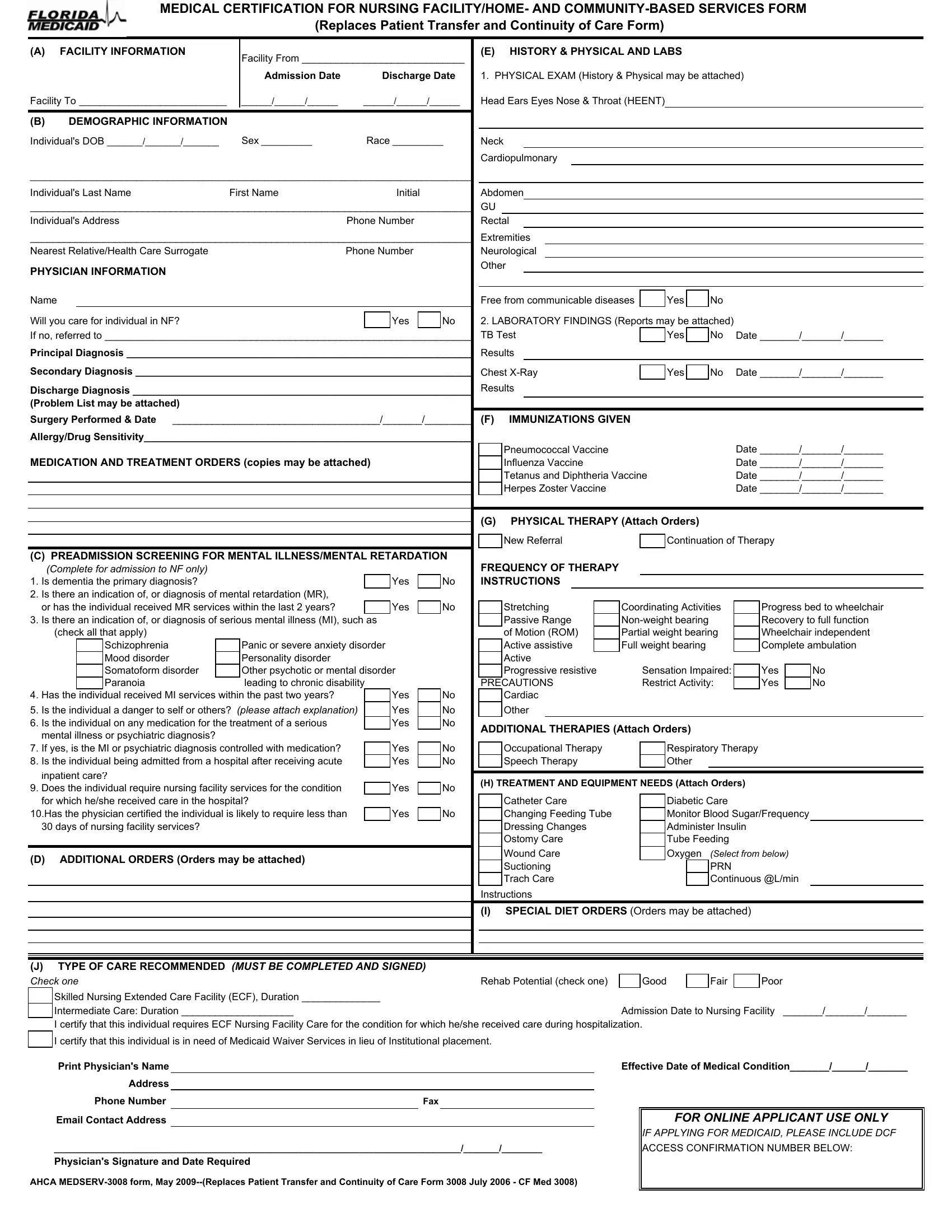
2. Once your current task is complete, take the next step – fill out all of these fields - AllergyDrug Sensitivity, MEDICATION AND TREATMENT ORDERS, C PREADMISSION SCREENING FOR, Yes, Yes, check all that apply, Schizophrenia Mood disorder, Panic or severe anxiety disorder, Has the individual received MI, Is the individual a danger to, inpatient care Does the, Yes, Yes Yes, Yes Yes, and Yes with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
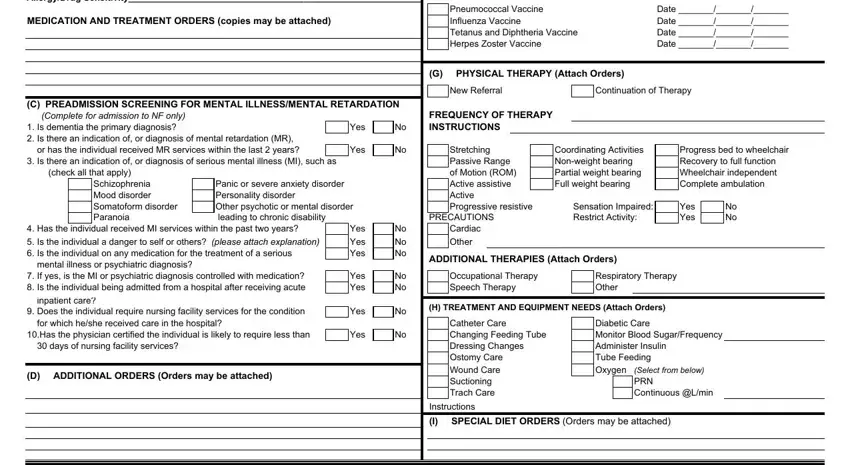
3. Within this step, have a look at J TYPE OF CARE RECOMMENDED MUST BE, Rehab Potential check one, Good, Fair, Poor, Skilled Nursing Extended Care, Admission Date to Nursing Facility, I certify that this individual is, Print Physicians Name, Address, Phone Number, Email Contact Address, Fax, Physicians Signature and Date, and AHCA MEDSERV form May Replaces. Each one of these need to be filled in with greatest accuracy.
It is easy to make an error while filling out your Email Contact Address, hence make sure you take another look before you submit it.
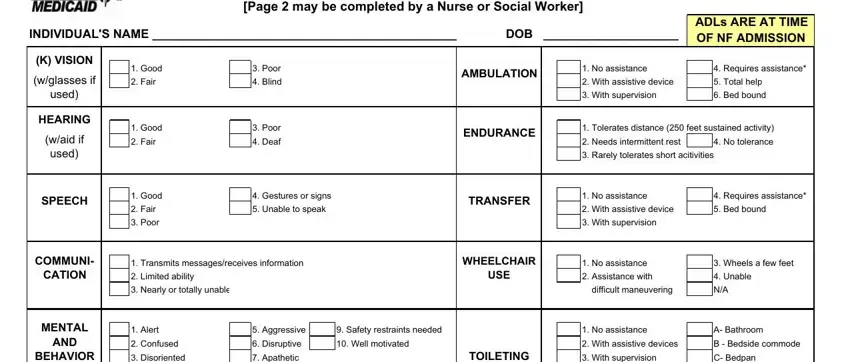
4. To move onward, this part will require filling out several blank fields. Examples of these are NURSINGSOCIAL WORK ASSESSMENT, Page may be completed by a Nurse, INDIVIDUALS NAME DOB, ADLs ARE AT TIME OF NF ADMISSION, K VISION, wglasses if, used, HEARING, waid if used, SPEECH, Good, Fair, Good, Fair, and Good, which you'll find vital to going forward with this particular document.
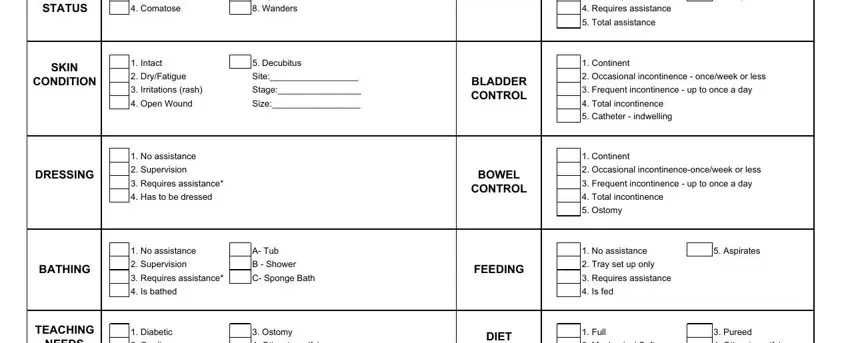
5. To conclude your document, this particular part has some extra blank fields. Entering BEHAVIOR, STATUS, Disoriented, Comatose, Apathetic, Wanders, TOILETING, With supervision, C Bedpan, Requires assistance, Total assistance, SKIN, CONDITION, Intact, and DryFatigue is going to wrap up everything and you're going to be done in no time!
Step 3: After you've looked over the details you filled in, press "Done" to finalize your form at FormsPal. Get your florida medical nursing form as soon as you sign up at FormsPal for a free trial. Conveniently view the pdf form in your FormsPal account, together with any edits and changes being automatically saved! Whenever you work with FormsPal, you can fill out forms without having to worry about data incidents or data entries being distributed. Our secure system ensures that your private information is kept safely.