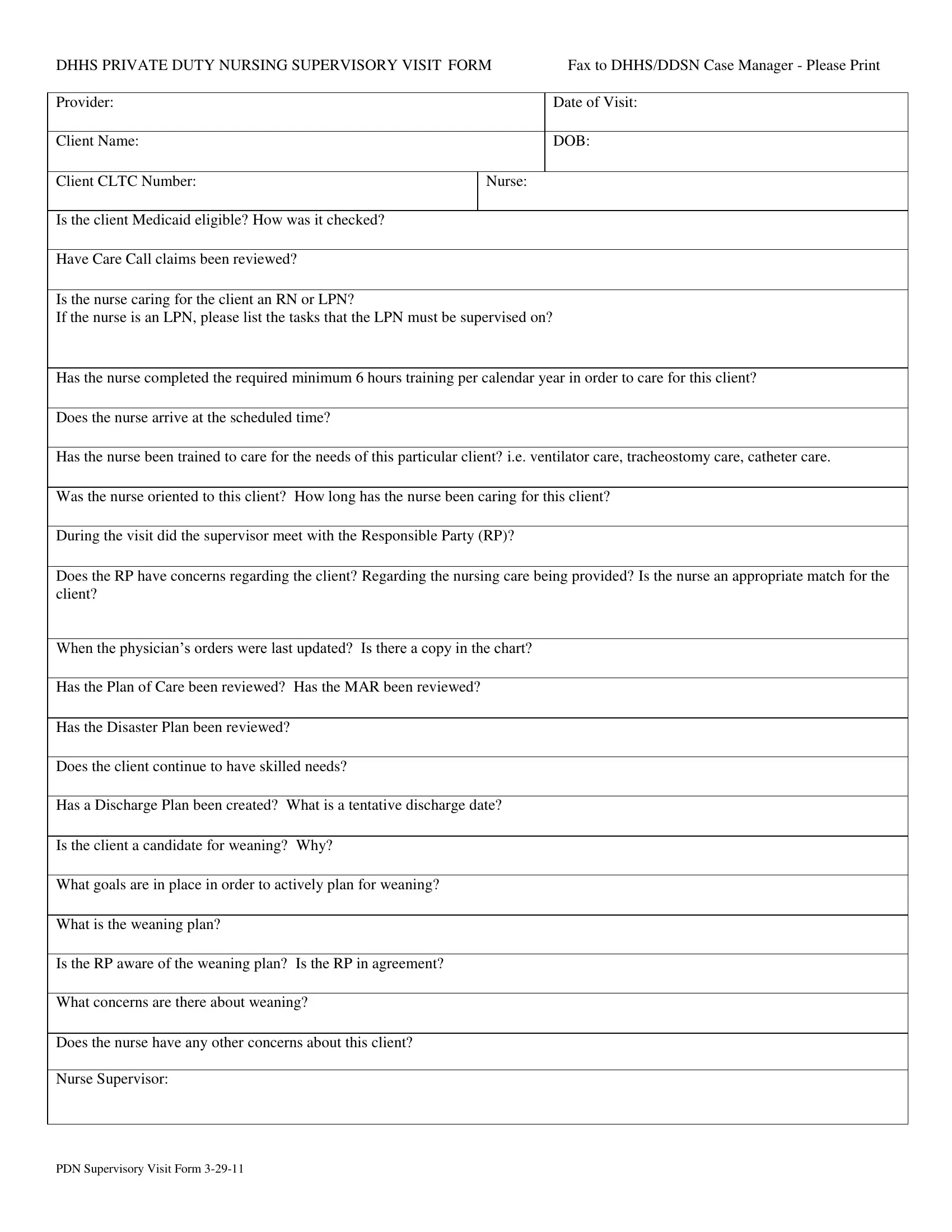
In the landscape of healthcare, meticulous documentation ensures that patients receive consistent, high-quality care tailored to their specific needs. Among the critical documents within this ecosystem is the Nursing Supervisory Visit Form, an essential tool facilitated by the Department of Health and Human Services (DHHS) for private duty nursing. This comprehensive form serves as a linchpin in both the assessment and oversight of patient care, addressing various aspects such as the verification of a client’s Medicaid eligibility, the review of care call claims, and the delineation of tasks for which a Licensed Practical Nurse (LPN) requires supervision versus those within the purview of a Registered Nurse (RN). It further probes into the adequacy of nurse training—both general and client-specific, punctuality, and the effectiveness of the orientation to the client's needs. The document encourages a holistic review, including an evaluation of the current Plan of Care, Medication Administration Record (MAR), disaster preparedness, and even the contemplation of discharge planning and weaning from services, if applicable. Through this form, supervisors are not just assessing the professional competency and performance of the nursing staff but are also engaging in a dynamic dialogue with the Responsible Party (RP) to ensure the client's care plan remains appropriate and responsive to their evolving needs. Thus, the Nursing Supervisory Visit Form stands as a testament to the ongoing commitment to quality care and regulatory compliance within the realm of private duty nursing.
| Question | Answer |
|---|---|
| Form Name | Nursing Supervisory Visit Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 26 |
| Avg. time to fill out | 5 min 27 sec |
| Other names | DDSN, home hospice nurse supervisory visit form, DHHS, PDN |
DHHS PRIVATE DUTY NURSING SUPERVISORY VISIT FORM |
Fax to DHHS/DDSN Case Manager - Please Print |
|
|
|
|
Provider: |
|
Date of Visit: |
|
|
|
Client Name: |
|
DOB: |
|
|
|
Client CLTC Number: |
Nurse: |
|
|
|
|
Is the client Medicaid eligible? How was it checked? |
|
|
|
|
|
Have Care Call claims been reviewed? |
|
|
|
|
|
Is the nurse caring for the client an RN or LPN? |
|
|
If the nurse is an LPN, please list the tasks that the LPN must be supervised on?
Has the nurse completed the required minimum 6 hours training per calendar year in order to care for this client?
Does the nurse arrive at the scheduled time?
Has the nurse been trained to care for the needs of this particular client? i.e. ventilator care, tracheostomy care, catheter care.
Was the nurse oriented to this client? How long has the nurse been caring for this client?
During the visit did the supervisor meet with the Responsible Party (RP)?
Does the RP have concerns regarding the client? Regarding the nursing care being provided? Is the nurse an appropriate match for the client?
When the physician’s orders were last updated? Is there a copy in the chart?
Has the Plan of Care been reviewed? Has the MAR been reviewed?
Has the Disaster Plan been reviewed?
Does the client continue to have skilled needs?
Has a Discharge Plan been created? What is a tentative discharge date?
Is the client a candidate for weaning? Why?
What goals are in place in order to actively plan for weaning?
What is the weaning plan?
Is the RP aware of the weaning plan? Is the RP in agreement?
What concerns are there about weaning?
Does the nurse have any other concerns about this client?
Nurse Supervisor:
PDN Supervisory Visit Form