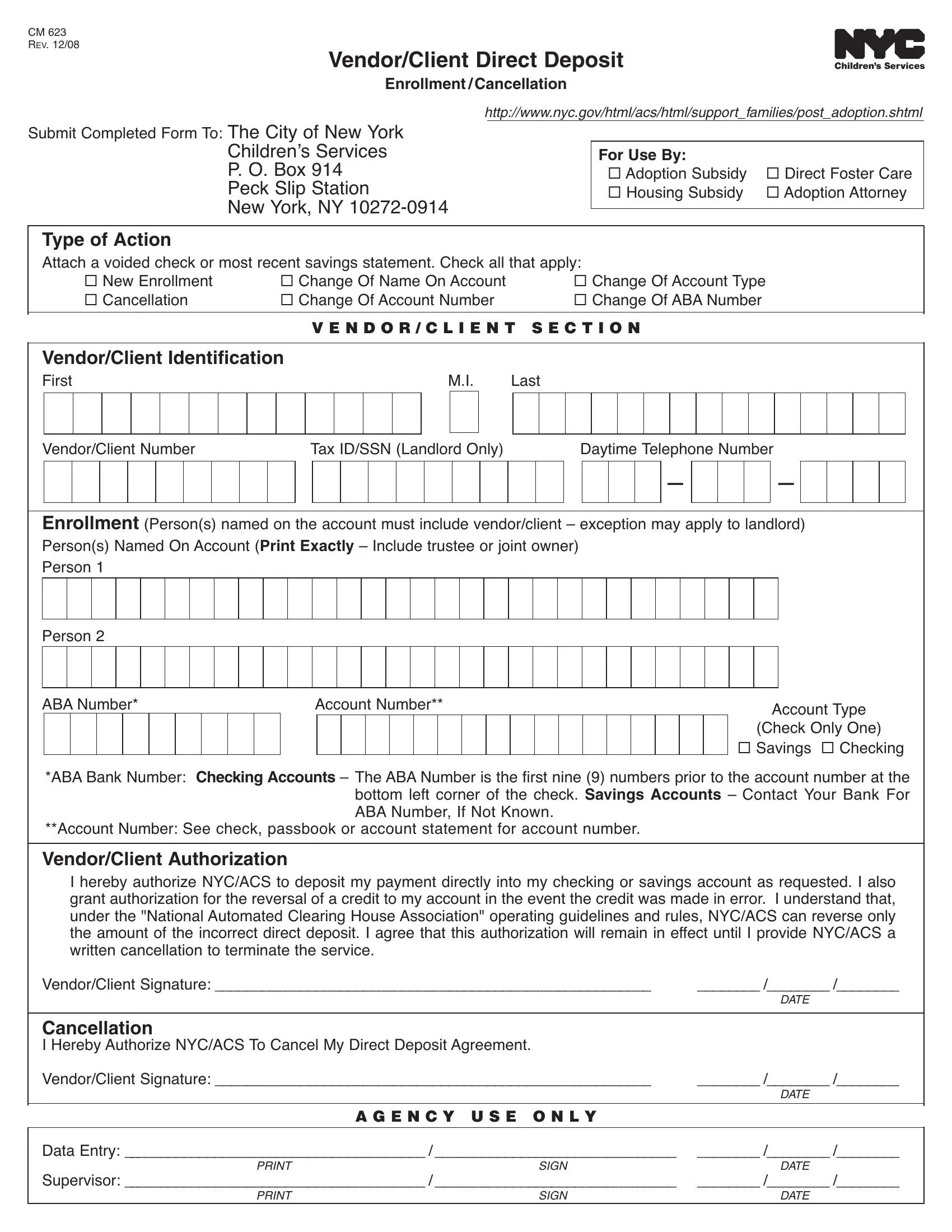
In the bustling cityscape of New York City, financial transactions and bureaucratic processes are streamlined for efficiency, ensuring that vendors and clients engaged with city services experience seamlessness in payment methodologies. At the heart of this streamlined process lies the NYC CM 623 form, a crucial document designed for the purpose of Vendor/Client Direct Deposit Enrollment or Cancellation. This form plays a pivotal role for individuals or entities receiving payments from The City of New York Children’s Services, accommodating a variety of situations including adoption subsidies, direct foster care payments, housing subsidies, and transactions with adoption attorneys. It offers options for new enrollments, changes in account details such as name, account type, or account number, and cancellations, requiring the attachment of a voided check or the most recent savings account statement for verification. The form mandates thorough identification of the vendor or client through specified fields, ensuring accurate processing. Furthermore, it stands as a testament to the city’s commitment to operational efficiency and security, requiring vendor or client authorization to allow NYC/ACS (New York City/Administration for Children’s Services) to directly deposit or reverse payments to declared financial accounts, underlined by the conditions set by the National Automated Clearing House Association. The CM 623 form encapsulates the crucial steps for seamless financial transactions, embodying the principle of precision and care in handling personal and sensitive information in the realm of public services.
| Question | Answer |
|---|---|
| Form Name | Nyc Form Cm 623 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | direct_deposit_ form nyc acs employee direct deposet form |
CM 623
REV. 12/08
Vendor/Client Direct Deposit
Enrollment / Cancellation
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
http://www.nyc.gov/html/acs/html/support_families/post_adoption.shtml |
|||||||||||||||||||||||||||
Submit Completed Form To: TheCityofNewYork |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
ChildrenʼsServices |
|
|
|
|
|
|
For Use By: |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
P. O. Box914 |
|
|
|
|
|
|
AdoptionSubsidy |
DirectFosterCare |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
PeckSlipStation |
|
|
|
|
|
|
HousingSubsidy |
AdoptionAttorney |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Action |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Attach a voided check or most recent savings statement. Check all that apply: |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||
|
|
NewEnrollment |
|
|
|
|
ChangeOfNameOnAccount |
|
|
|
|
ChangeOfAccountType |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
Cancellation |
|
|
|
|
ChangeOfAccountNumber |
|
|
|
|
ChangeOfABANumber |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
V E N D O R / C L I E N T S E C T I O N |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vendor/Client Identification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
First |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M.I. |
Last |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vendor/ClientNumber |
|
|
|
|
|
|
TaxID/SSN(LandlordOnly) |
|
|
|
|
DaytimeTelephoneNumber |
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– |
|
|
|
|
|
|
|
|
– |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Enrollment (Person(s)namedontheaccountmustincludevendor/client – exceptionmayapplytolandlord)
Person(s)NamedOnAccount(Print Exactly – Includetrusteeorjointowner)
Person1
Person2
ABANumber* |
|
|
|
|
|
AccountNumber** |
|
|
|
|
|
|
|
|
|
|
|
AccountType |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CheckOnlyOne) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Savings Checking |
*ABABankNumber: Checking Accounts – TheABANumberisthefirstnine(9)numberspriortotheaccountnumberatthe bottom left corner of the check. Savings Accounts – Contact Your Bank For ABANumber, If Not Known.
**AccountNumber:See check, passbook or account statement for account number.
Vendor/Client Authorization
I hereby authorize NYC/ACS to deposit my payment directly into my checking or savings account as requested. I also grantauthorizationforthereversalofacredittomyaccountintheeventthecreditwasmadeinerror. Iunderstandthat, under the "NationalAutomated Clearing HouseAssociation" operating guidelines and rules, NYC/ACS canreverseonly the amount of the incorrect direct deposit. I agree that this authorization will remain in effect until I provide NYC/ACS a writtencancellationtoterminatetheservice.
Vendor/ClientSignature: ________________________________________________________ |
________/________/________ |
|
DATE |
Cancellation
IHerebyAuthorizeNYC/ACSToCancelMyDirectDepositAgreement.
Vendor/ClientSignature: ________________________________________________________ |
________/________/________ |
|
|
|
DATE |
|
|
|
|
A G E N C Y U S E O N L Y |
|
|
|
|
DataEntry: _______________________________________/_______________________________ |
________/________/________ |
|
SIGN |
DATE |
|
Supervisor: _______________________________________/_______________________________ |
________/________/________ |
|
SIGN |
DATE |
|