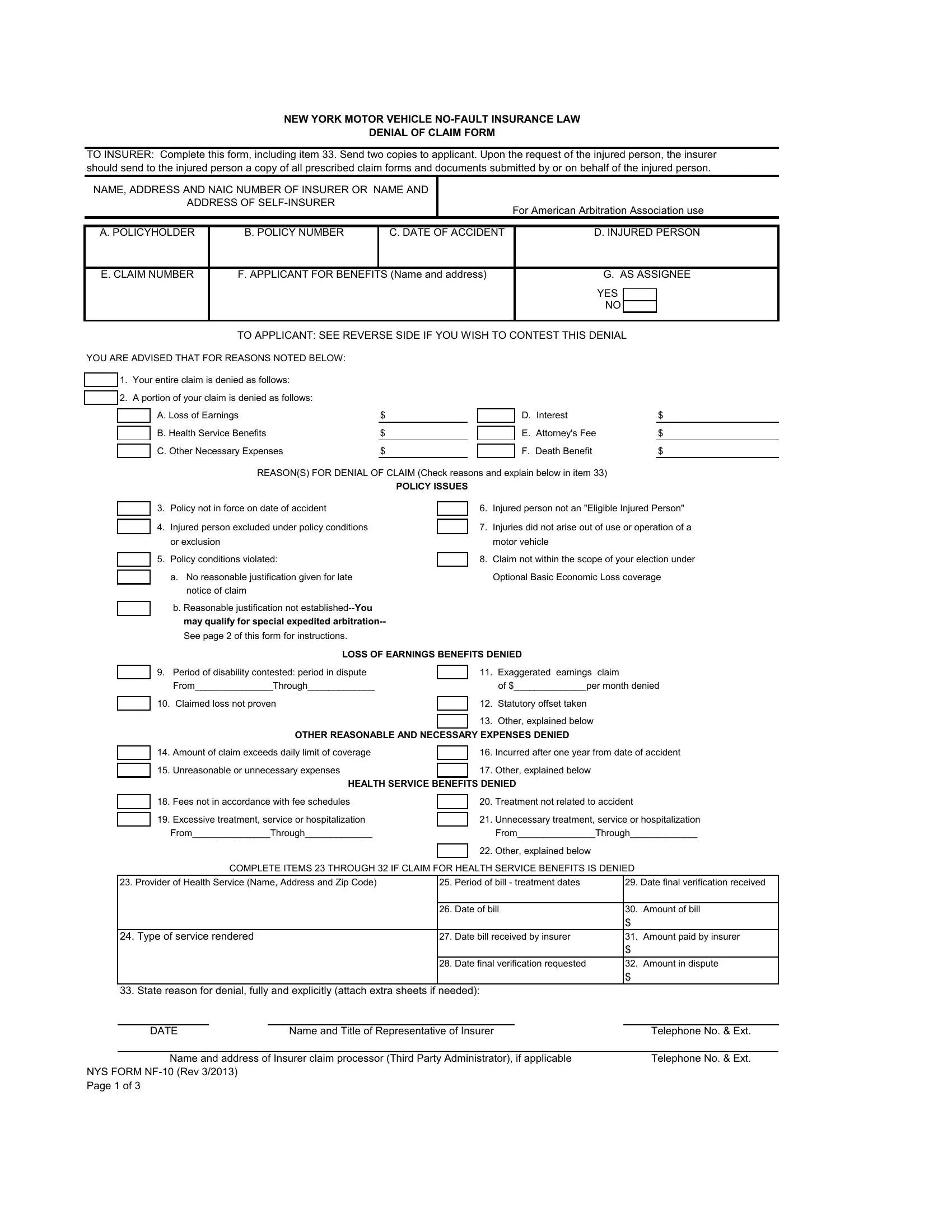
The New York State (NYS) NF-10 form plays a pivotal role in the realm of motor vehicle no-fault insurance, marking a critical juncture for policyholders and claimants navigating the complexities of claim denials. Designed to communicate an insurer's refusal to cover a claim under the New York Motor Vehicle No-Fault Insurance Law, this form ensures that clear, written notification is provided to the applicant or their assignee. It details the reasons for denial, whether it be for the entire claim or just a portion, specifying issues such as policy validity, policy exclusions, late notifications, and discrepancies in claimed losses, among others. The form not only outlines the grounds of the denial—ranging from loss of earnings and unreasonable medical expenses to disputes over the necessity and appropriateness of health services—but it also facilitates recourse for the aggrieved party. Through detailed instructions, it guides claimants on how to challenge the denial, whether by appealing to the New York State Department of Financial Services, engaging in arbitration with the American Arbitration Association, or pursuing legal action. In its essence, the NYS NF-10 form embodies the procedural fairness and transparency that underpin the adjudication of no-fault insurance claims, providing a structured pathway for both claim resolution and dispute escalation.
| Question | Answer |
|---|---|
| Form Name | Nys Form Nf 10 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | ny nf10, ny nf10 form, nf10, new york nf 10 form |
NEW YORK MOTOR VEHICLE
DENIAL OF CLAIM FORM
TO INSURER: Complete this form, including item 33. Send two copies to applicant. Upon the request of the injured person, the insurer should send to the injured person a copy of all prescribed claim forms and documents submitted by or on behalf of the injured person.
NAME, ADDRESS AND NAIC NUMBER OF INSURER OR NAME AND
ADDRESS OF
For American Arbitration Association use
A. POLICYHOLDER |
B. POLICY NUMBER |
C. DATE OF ACCIDENT |
D. INJURED PERSON |
||||||
|
|
|
|
|
|||||
E. CLAIM NUMBER |
F. APPLICANT FOR BENEFITS (Name and address) |
G. AS ASSIGNEE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
|
|
|
|
|
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO APPLICANT: SEE REVERSE SIDE IF YOU WISH TO CONTEST THIS DENIAL |
|
|||||
YOU ARE ADVISED THAT FOR REASONS NOTED BELOW: |
|
|
|
|
|
|
|||
|
1. Your entire claim is denied as follows: |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||
|
2. A portion of your claim is denied as follows: |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||
|
|
A. Loss of Earnings |
$ |
|
|
D. Interest |
$ |
||
|
|
|
|
||||||
|
|
B. Health Service Benefits |
$ |
|
|
E. Attorney's Fee |
$ |
||
|
|
|
|
||||||
|
|
C. Other Necessary Expenses |
$ |
|
|
F. Death Benefit |
$ |
||
|
|
|
|
||||||
|
|
|
REASON(S) FOR DENIAL OF CLAIM (Check reasons and explain below in item 33) |
|
|||||
|
|
|
|
POLICY ISSUES |
|
|
|
||
3.Policy not in force on date of accident
4.Injured person excluded under policy conditions or exclusion
5.Policy conditions violated:
a.No reasonable justification given for late notice of claim
b.Reasonable justification not
6.Injured person not an "Eligible Injured Person"
7.Injuries did not arise out of use or operation of a motor vehicle
8.Claim not within the scope of your election under Optional Basic Economic Loss coverage
LOSS OF EARNINGS BENEFITS DENIED
9.Period of disability contested: period in dispute From_______________Through_____________
10.Claimed loss not proven
11.Exaggerated earnings claim
of $______________per month denied
12.Statutory offset taken
13.Other, explained below
OTHER REASONABLE AND NECESSARY EXPENSES DENIED
14.Amount of claim exceeds daily limit of coverage
15.Unreasonable or unnecessary expenses
16.Incurred after one year from date of accident
17.Other, explained below
|
HEALTH SERVICE BENEFITS DENIED |
|||
18. |
Fees not in accordance with fee schedules |
|
20. |
Treatment not related to accident |
|
||||
19. |
Excessive treatment, service or hospitalization |
|
Unnecessary treatment, service or hospitalization |
|
|
21. |
|||
|
From_______________Through_____________ |
|
|
From_______________Through_____________ |
|
|
|
Other, explained below |
|
|
|
|
22. |
|
COMPLETE ITEMS 23 THROUGH 32 IF CLAIM FOR HEALTH SERVICE BENEFITS IS DENIED
23. Provider of Health Service (Name, Address and Zip Code) |
25. |
Period of bill - treatment dates |
29. Date final verification received |
|
|
|
|
|
|
|
26. |
Date of bill |
30. |
Amount of bill |
|
|
|
$ |
|
24. Type of service rendered |
27. |
Date bill received by insurer |
31. |
Amount paid by insurer |
|
|
|
$ |
|
|
28. |
Date final verification requested |
32. |
Amount in dispute |
|
|
|
$ |
|
33. State reason for denial, fully and explicitly (attach extra sheets if needed):
DATE |
|
Name and Title of Representative of Insurer |
|
Telephone No. & Ext. |
|
|
|||
Name and address of Insurer claim processor (Third Party Administrator), if applicable |
Telephone No. & Ext. |
|||
NYS FORM
Page 1 of 3
DENIAL OF CLAIM FORM
IF YOU WISH TO CONTEST THIS DENIAL, YOU HAVE THE FOLLOWING OPTIONS:
1.Should you wish to take this matter up with the New York State Department of Financial Services, you may file with the Department either on its website at http://www.dfs.ny.gov/consumer/fileacomplaint.htm or you may write to or visit the Consumer Assistance Unit, Financial Frauds and Consumer Protection Division, New York State Department of Financial Services, at: One State Street, New York, NY 10004; One Commerce Plaza, Albany, NY 12257; 163B Mineola Boulevard, Mineola, NY 11501, or Walter J. Mahoney Office Building, 65 Court Street, Buffalo, NY 14202.
Although the Department of Financial Services will attempt to resolve disputed claims, it cannot order or require an insurer to pay a disputed claim. If you wish to file a written complaint, send one copy of this Denial of Claim Form with copies of other pertinent documents with a letter fully explaining your complaint to the Department of Financial Services at one of the above addresses.
If you choose this option, you may at a later date still submit this dispute to arbitration or bring a lawsuit; or
2.You may submit this dispute to arbitration. If you wish to submit this claim to arbitration, then mail or
together with a $40 filing fee, payable by check, money order, or credit card to the American Arbitration Association (AAA) to:
AMERICAN ARBITRATION ASSOCIATION (AAA)
NEW YORK INSURANCE CASE MANAGEMENT CENTER 120 BROADWAY
NEW YORK, NEW YORK 10271
nyicmc.filingsubmissions@adr.org
Please contact the American Arbitration Association's customer service department at (917)
A complete copy of this filing, listing all bills and proofs as well as a table of contents listing your submissions must be provided to the AAA and the insurer at the time of filing for arbitration. The filing must be complete with all necessary documentation, as any late submission may not be admissible at arbitration. The filing fee will be returned to you if the arbitrator awards you any portion of your claim. However, you may be assessed the costs of the arbitration proceeding if the arbitrator finds your claim to be frivolous, without factual or legal merit or was filed for the purpose of harassing the respondent. The decision of an arbitrator is binding, except for limited grounds for review set forth in the Law and regulations promulgated thereunder.
If you are contesting the denial of claim and wish to submit the dispute to arbitration, state on accompanying sheets the reason(s) you believe the denied or overdue benefits should be paid. Attach proof of disability and verification of loss of earnings in dispute, sign below, and send the completed form to the American Arbitration Association at the address given in item 2 above.
Loss of earnings: |
Date claim made:_____________________ |
Gross earnings per month $______________________ |
Period of dispute: |
From ___________ Through _____________ |
Amount claimed: $_____________________________ |
Health Services: (Attach bills in dispute and list each one separately)
Name of Provider(s) |
Date of Service |
Amount of Bill |
|
|
|
Amount in Dispute
Date Claim Mailed
Other Necessary Expenses: (Attach bills in dispute and list each one separately)
Type of Expenses Claimed |
Amount Claimed |
Date Incurred |
|
|
|
Date Claim Mailed
Amount in Dispute
Other: (attach additional sheet if necessary)
·Upon your request, if you file for arbitration within 90 days of the date of this denial or the claim becoming overdue, your case will be scheduled for arbitration on a priority basis.
·You qualify for special expedited arbitration if the insurer has determined that your written justification for submitting late notice of claim failed to meet a “reasonableness standard”. Your specific request for special expedited arbitration must be filed within 30 days of the date of denial. Your filing must be complete and contain all information that you are submitting at the time of filing.
NYS FORM
Page 2 of 3
DENIAL OF CLAIM FORM
3.You may bring a lawsuit to recover the amount of benefits you claim to be entitled to.
THE UNDERSIGNED AFFIRMS AND CERTIFIES AS TRUE UNDER THE PENALTY OF PERJURY THAT THIS FILING IS BEING MADE IN GOOD FAITH AND THAT UPON INFORMATION, BELIEF AND REASONABLE INQUIRY THE DOCUMENTS BEING SUBMITTED HEREWITH ARE NOT FRAUDULENT AND THAT EXACT COPIES OF ALL DOCUMENTS PROVIDED HEREWITH HAVE BEEN MAILED TO THE INSURER AGAINST WHOM THE ARBITRATION IS BEING REQUESTED. UNLESS DISCLOSED WITH THIS SUBMISSION, THE DISPUTED AMOUNTS REMAIN UNPAID TO THE APPLICANT BY ANY PAYOR AND THERE HAS BEEN NO OTHER FILING OF AN ARBITRATION REQUEST OR LAWSUIT TO RESOLVE THE DISPUTED MATTERS CONTAINED IN THIS SUBMISSION.
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR OTHER PERSON FILES AN APPLICATION FOR COMMERCIAL INSURANCE OR A STATEMENT OF CLAIM FOR ANY COMMERCIAL OR PERSONAL INSURANCE BENEFITS CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO, AND ANY PERSON WHO, IN CONNECTION WITH SUCH APPLICATION OR CLAIM, KNOWINGLY MAKES OR KNOWINGLY ASSISTS, ABETS, SOLICITS OR CONSPIRES WITH ANOTHER TO MAKE A FALSE REPORT OF THE THEFT, DESTRUCTION, DAMAGE OR CONVERSION OF ANY MOTOR VEHICLE TO A LAW ENFORCEMENT AGENCY, THE DEPARTMENT OF MOTOR VEHICLES OR AN INSURANCE COMPANY, COMMITS A FRAUDULENT INSURANCE ACT, WHICH IS A CRIME, AND SHALL ALSO BE SUBJECT TO A CIVIL PENALTY NOT TO EXCEED FIVE THOUSAND DOLLARS AND THE VALUE OF THE SUBJECT MOTOR VEHICLE OR STATED CLAIM FOR EACH VIOLATION.
ARBITRATION REQUESTED BY:
LAST NAME |
FIRST NAME |
NAME OF LAW FIRM, IF ANY |
|
|
TELEPHONE NUMBER: |
|
|
|
|
|
|
|
|
|
FAX NUMBER: |
|
|
|
|
|
|
|
|
|
EMAIL ADDRESS: |
|
|
|
|
|
|
ADDRESS |
|
|
|
|
ARE YOU AN ATTORNEY? |
|
DATE |
|
|
YES |
|
|
|
|
NO |
|
|
SIGNATURE |
|
|
|
|
IMPORTANT NOTICE TO APPLICANT
If box number 3 ("Policy not in force on date of accident") on the front of this form is checked as a reason for this denial, you may be entitled to
your best interest to contact the M.V.A.I.C. immediately and file such an affidavit, even if you intend to contest this denial.
NYS FORM