This PDF editor was made to be so simple as possible. While you keep up with these steps, the procedure for filling out the 7210 or application file will undoubtedly be effortless.
Step 1: Hit the button "Get form here" to open it.
Step 2: Now you will be on your document edit page. You'll be able to add, transform, highlight, check, cross, add or erase areas or phrases.
For you to get the form, provide the data the program will require you to for each of the following areas:
Type in the demanded details in the STEP, Legal name first middle last and, Maiden or other names used first, Social Security number SSN An, SSN, No Applied for SSN Newborn Dont, Birthdate MMDDYYYY, Sex, Phone number Home Work Cell, Male Female, Do you live in Oregon Answer yes, Only answer if you are applying, Email address, Home address skip to if you dont, and ApartmentUnit segment.
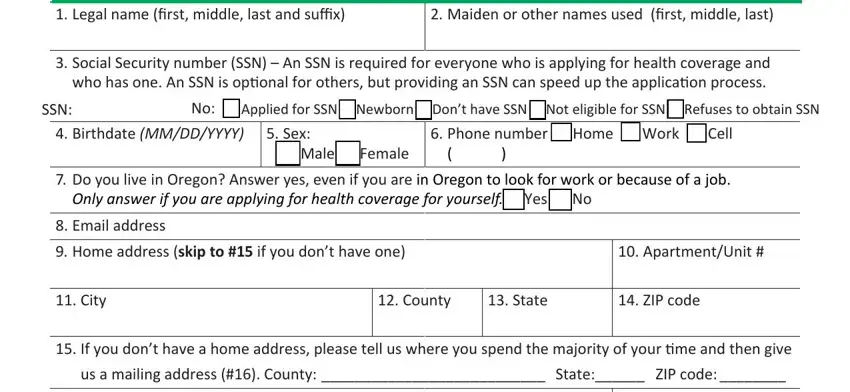
The program will require details to instantly fill in the box Mailing address only required if, ApartmentUnit, City, State, and ZIP code.

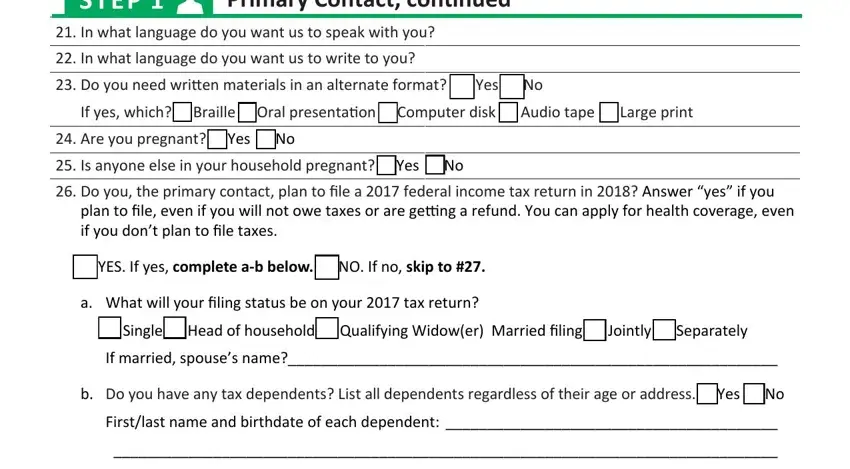
In the field STEP, Primary Contact continued, In what language do you want us, In what language do you want us, Do you need written materials in, If yes which Braille Oral, Are you pregnant Yes No Is, Do you the primary contact plan, plan to file even if you will not, YES If yes complete ab below NO, What will your filing status be on, Single Head of household, If married spouses name, Do you have any tax dependents, and Firstlast name and birthdate of, list the rights and obligations of the parties.
Check the areas Note for each person listed as a, Are you claimed as a dependent on, If yes list firstlast name and, How are you related to the tax, If HispanicLatino ethnicity, Mexican Mexican American, Race check all that apply, American Indian or Alaska Native, Filipino Guamanian or Chamorro, Other Pacific Islander Samoan, Is your tax filing information, YES NO If no complete Appendix D, Are you applying for health, coverage, and YES If yes go to NO If no skip and thereafter fill them in.
Step 3: Once you've clicked the Done button, your document is going to be available for upload to every gadget or email address you identify.
Step 4: It may be simpler to keep duplicates of your document. You can be sure that we will not share or see your data.
