In the realm of navigating workers' compensation in Ohio, the BWC 1389 form plays a crucial role in how individuals manage their claims and personal information. This form is essentially an authorization to release information, facilitating communication between the Bureau of Workers' Compensation (BWC) and designated parties chosen by the claimant. Designed to aid those who may need assistance whether due to the complexities of their cases or personal circumstances, it empowers claimants to designate family members, friends, or even professionals involved in their care or claim management to receive information directly from the BWC. The stipulated validity of this authorization extends to one year from the date it is signed, ensuring that permissions are current and reflect the claimant's present wishes. Essential details such as the claimant’s name, date of birth, claim number, and contact information, along with the authorized party’s similar details and the specific types of information to be disclosed, including claims status, medical documentation, and wage or payment details, are all integral parts of the form. Particularly noteworthy is the requirement for a signature from the injured worker, their guardian, or personal representative, along with a description of the representative’s authority, underscoring the form's role in safeguarding the claimant's informational privacy while facilitating necessary support.
| Question | Answer |
|---|---|
| Form Name | Ohio Form Bwc 1389 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | c 257 ohio bureau of workers comp authorization to release information pdf |
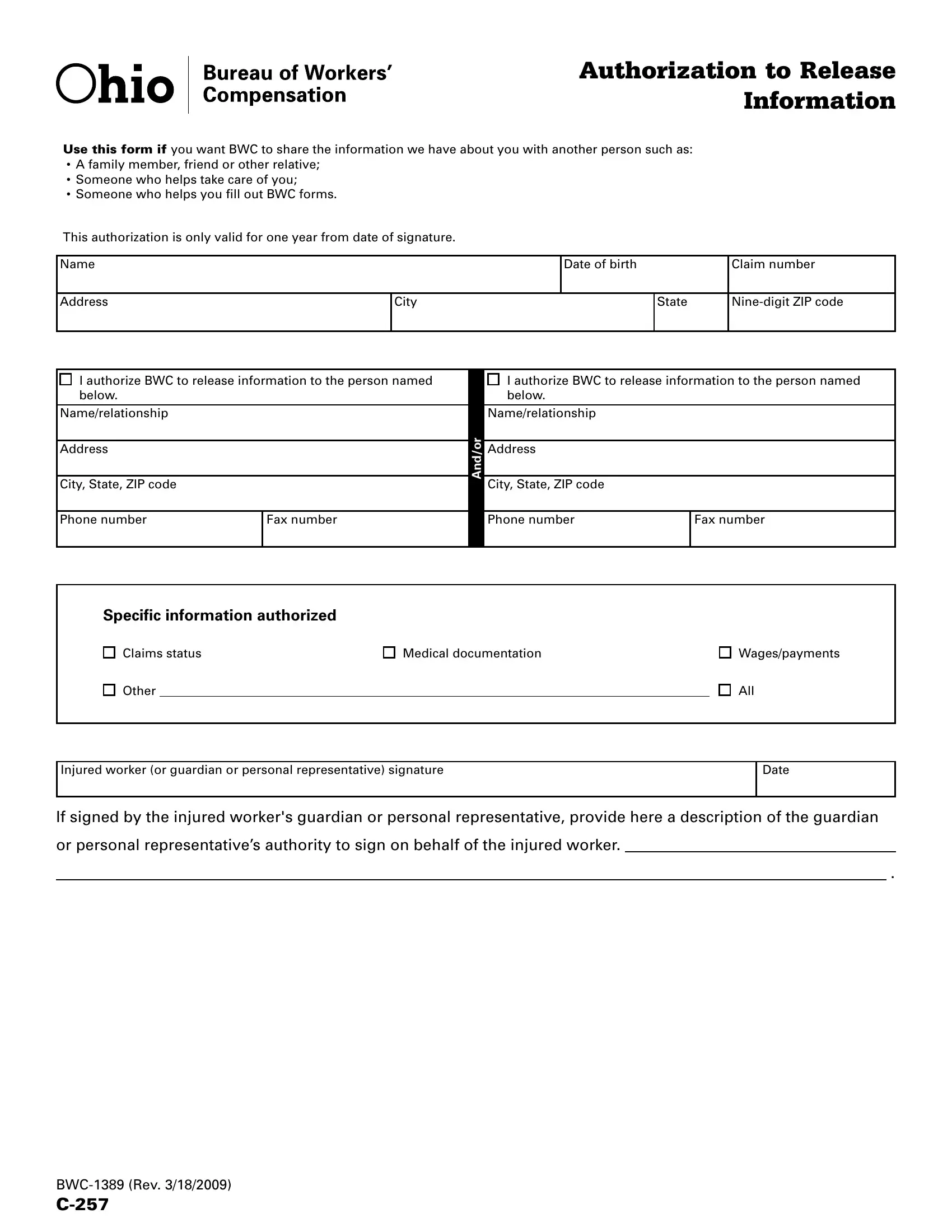
AUTHORIZATION TO RELEASE
INFORMATION
USE THIS FORM IF you want BWC to share the information we have about you with another person such as:
•A family member, friend or other relative;
•Someone who helps take care of you;
•Someone who helps you ill out BWC forms.
This authorization is only valid for one year from date of signature.
Name |
Date of birth |
Claim number |
|
|
|
Address
City
State
I authorize BWC to release information to the person named |
|
I authorize BWC to release information to the person named |
||
below. |
|
|
below. |
|
Name/relationship |
|
|
Name/relationship |
|
|
|
And/or |
|
|
Address |
|
Address |
|
|
|
|
|
|
|
City, State, ZIP code |
|
City, State, ZIP code |
|
|
|
|
|
||
|
|
|
|
|
Phone number |
Fax number |
|
Phone number |
Fax number |
|
|
|
|
|
Specific information authorized
Claims status
Other
Medical documentation
Wages/payments
All
Injured worker (or guardian or personal representative) signature
Date
If signed by the injured worker's guardian or personal representative, provide here a description of the guardian
or personal representative’s authority to sign on behalf of the injured worker.
.