In the landscape of workers' compensation in Ohio, the BWC 3907 form plays a pivotal role in the management of cases involving injured workers who are receiving temporary total disability compensation. Navigating through the legal requirements set forth by Section 4123.53 (B) of the Ohio Revised Code, this document facilitates a critical exception process whereby the mandatory medical examination, typically required after 90 consecutive days of such compensation, can be waived. Predicated on circumstances such as the injured worker's hospitalization, pending surgery, or an imminent return to work, the waiver process underscores the importance of individual case assessment in determining the necessity of these examinations. Execution of the form necessitates involvement from multiple parties, including the employer or Bureau of Workers' Compensation (BWC) through an authorized representative, and may involve a recommendation from the BWC nurse. Decisions rendered by the BWC—whether to approve or deny the request for a waiver—are documented, underscoring the form's role as a critical piece of the administrative process within the broader context of supporting workers' recovery while ensuring accountability and oversight in the dispensation of disability compensation.
| Question | Answer |
|---|---|
| Form Name | Ohio Form Bwc 3907 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Ohio, bwc 337 form, bwc 337, Revised |
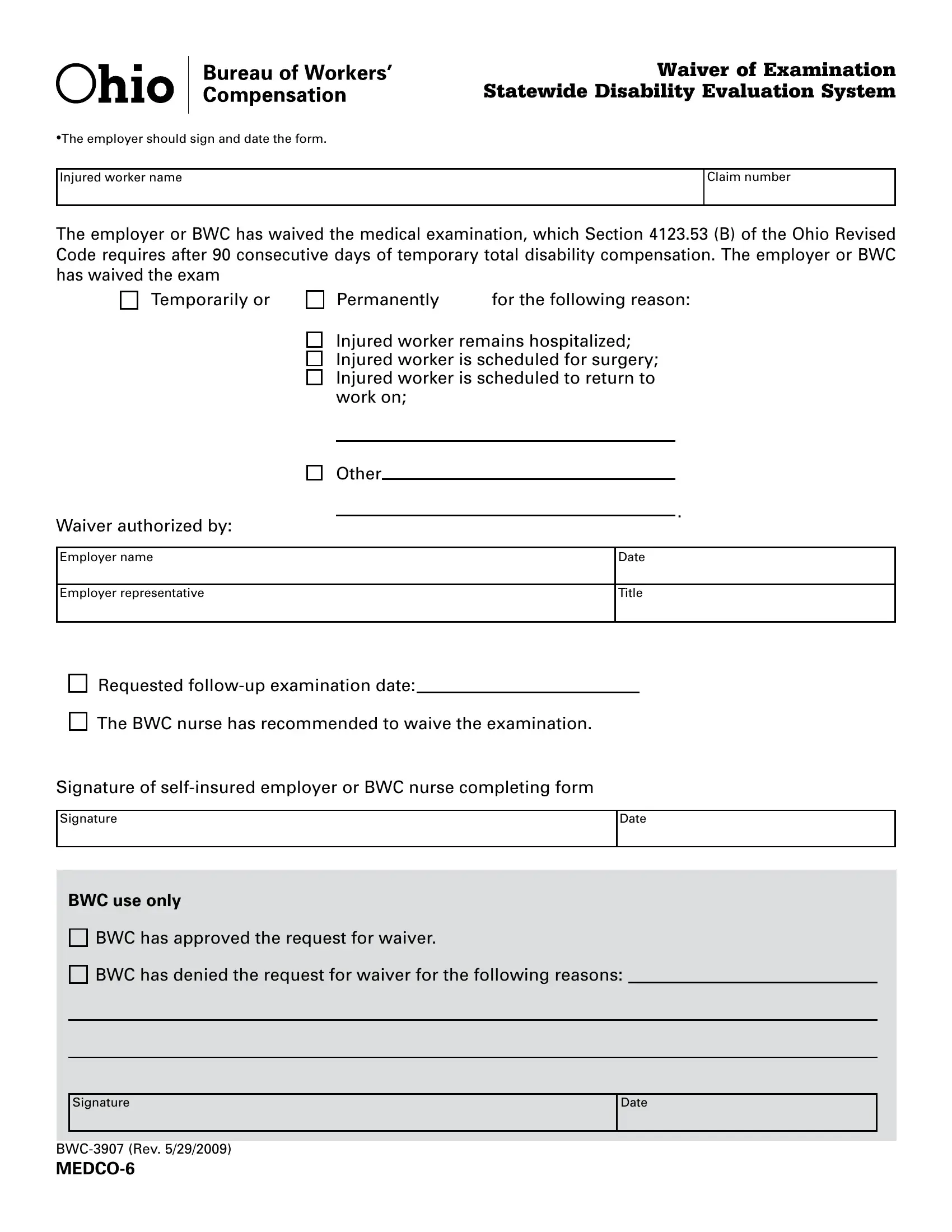
Waiver of Examination
Statewide Disability Evaluation System
•The employer should sign and date the form.
Injured worker name
Claim number
The employer or BWC has waived the medical examination, which Section 4123.53 (B) of the Ohio Revised
Code requires after 90 consecutive days of temporary total disability compensation. The employer or BWC
has waived the exam Temporarily or
Permanently |
for the following reason: |
Injured worker remains hospitalized; Injured worker is scheduled for surgery; Injured worker is scheduled to return to work on;
Other
.
Waiver authorized by:
Employer name
Date
Employer representative
Title
Requested
The BWC nurse has recommended to waive the examination.
Signature of
Signature
Date
BWC use only
BWC has approved the request for waiver.
BWC has denied the request for waiver for the following reasons:
Signature
Date