In today's healthcare landscape, the State of Oklahoma provides a crucial service through its Oklahoma Health Care Authority's Application for Family Planning Services, known colloquially as the FPWS 1 form. This form is designed for individuals aged 19 and older seeking access to family planning services under the SoonerPlan program. By requiring comprehensive input on household composition, contact information, verification of U.S. citizenship and identity, employment and income details, and insurance coverage, the application ensures that essential family planning resources are accessible to those in need. To streamline the process, applicants are guided to provide names as displayed on social security cards, diverse racial identifications, and detailed income sources, illustrating the state's dedication to accommodating a wide array of applicants. Additionally, the form underlines the importance of honesty and integrity, with specific sections dedicated to the rights and responsibilities of the applicant, including consent for the Oklahoma Health Care Authority to verify provided information and pursue necessary payments. This meticulous approach underscores Oklahoma's commitment to delivering equitable and comprehensive family planning services to its residents, emphasizing the necessity of accuracy and transparency in the application process.
| Question | Answer |
|---|---|
| Form Name | Oklahoma Form Fpws 1 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | SoonerCare, OKDHS, soonerplan, FPWS-1 |
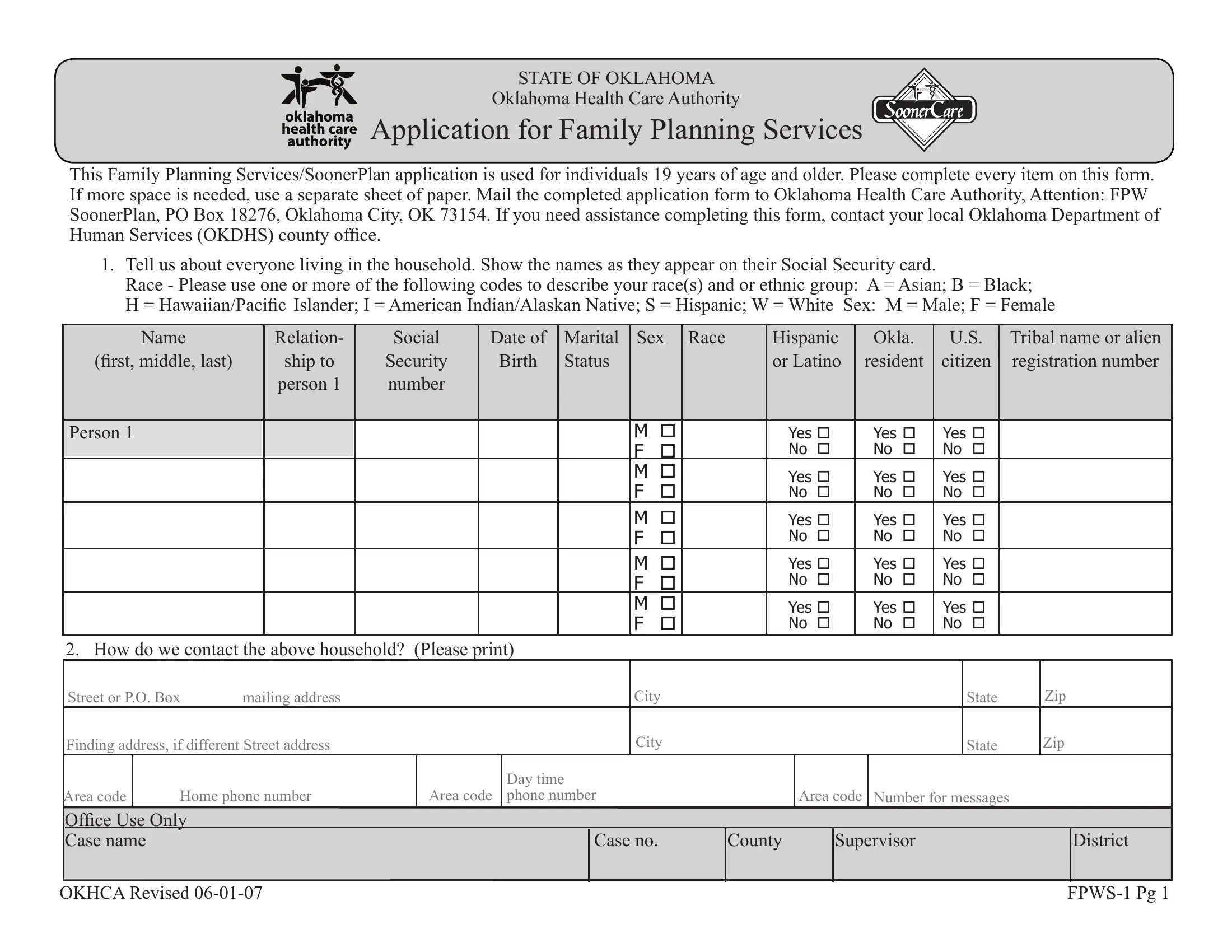
STATE OF OKLAHOMA
Oklahoma Health Care Authority
Application for Family Planning Services
This Family Planning Services/SoonerPlan application is used for individuals 19 years of age and older. Please complete every item on this form. If more space is needed, use a separate sheet of paper. Mail the completed application form to Oklahoma Health Care Authority, Attention: FPW SoonerPlan, PO Box 18276, Oklahoma City, OK 73154. If you need assistance completing this form, contact your local Oklahoma Department of Human Services (OKDHS) county ofice.
1.Tell us about everyone living in the household. Show the names as they appear on their Social Security card.
Race - Please use one or more of the following codes to describe your race(s) and or ethnic group: A = Asian; B = Black;
H = Hawaiian/Paciic Islander; I = American Indian/Alaskan Native; S = Hispanic; W = White Sex: M = Male; F = Female
NAME |
Relation- |
Social |
Date of |
Marital |
SEX |
Race |
Hispanic |
Okla. |
U.S. |
Tribal name or alien |
|
(irst, middle, last) |
ship to |
Security |
Birth |
Status |
|
|
|
or Latino |
resident |
citizen |
registration number |
|
person 1 |
number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Person 1 |
|
|
|
|
M |
|
YES |
YES |
YES |
|
|
|
|
|
|
|
F |
|
|
NO |
NO |
NO |
|
|
|
|
|
|
M |
|
YES |
YES |
YES |
|
|
|
|
|
|
|
F |
|
|
NO |
NO |
NO |
|
|
|
|
|
|
M |
|
YES |
YES |
YES |
|
|
|
|
|
|
|
F |
|
|
NO |
NO |
NO |
|
|
|
|
|
|
M |
|
YES |
YES |
YES |
|
|
|
|
|
|
|
F |
|
|
NO |
NO |
NO |
|
|
|
|
|
|
M |
|
YES |
YES |
YES |
|
|
|
|
|
|
|
F |
|
|
NO |
NO |
NO |
|
2. How do we contact the above household? (Please print)
|
|
Street or P.O. Box |
mailing address |
|
|
|
City |
|
|
|
|
State |
Zip |
||||
|
|
Finding address, if different Street address |
|
|
|
City |
|
|
|
|
|
Zip |
|||||
|
|
|
|
|
|
|
|
|
State |
||||||||
|
|
|
|
|
|
|
Day time |
|
|
|
|
|
|
|
|
||
|
Area code |
|
Home phone number |
Area code |
phone number |
|
Area code |
Number for messages |
|
|
|
||||||
|
Ofice Use Only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Case name |
|
|
|
|
Case no. |
County |
|
Supervisor |
|
|
District |
||||
OKHCA Revised |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||||||
Application for Family Planning Services |
3.For all U.S. citizens needing family planning services, identity must be veriied. Please mail a COPY of each person’s drivers license or government issued ID card with picture, school ID with picture, tribal CDIB card, or U.S. military ID card.
4.For all U.S. citizens needing family planning services, citizenship must also be veriied. Complete the information below. If available, mail a COPY of each person’s birth certiicate with this application.
Name (irst, middle, last) of the |
Name as shown on their birth |
County of |
State of |
Mother’s maiden name (irst, |
household member needing family |
certiicate (irst, middle, last) |
birth |
birth |
middle, last) as shown on the applicant's |
planning services |
|
|
|
birth certiicate |
|
|
|
|
|
Person 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. Is anyone in the household employed? Yes □ No □
Employer’s name, address and phone number
or self employment information
Who earns this money?
Gross earnings per pay period?
How often paid? (weekly, every other week, twice a month, monthly?)
OKHCA Revised |
Pg 2 |
Application for Family Planning Services |
6. Does anyone in the household get any other money or income? Yes No Some examples of other income are:
Social Security/SSI |
Other Pensions |
Support (alimony or child support) |
Annuities/Trust |
Worker’s Compensation |
Veteran’s Beneits |
Interest, such as C.D., stocks, bonds |
Railroad Retirement |
Military Allotment |
Royalties/Gas/Oil |
Money from friends, relatives, etc. |
Unemployment |
Rental |
Other, specify ____________________________________ |
|
|
If yes, give us the following information.
Name of person
money is for?
Source of money?
How much
money?
How often received?
7. Does anyone needing family planning services have health insurance? Yes No If yes, answer the following:
Insurance company name, address and phone number
Group or
policy
number
Person
covered
Type of coverage (major medical, dental, HMO, etc.)
Effective
date
Policy holder’s name and Social Security number
Relationship of
policy holder
to insured
OKHCA Revised |
Pg 3 |
Application for Family Planning Services |
Rights and Responsibilities
The information I give on this form is true and correct to the best of my knowledge. I realize if I give information that isn’t true OR if I withhold information, I can be lawfully punished for fraud or perjury. I may also have to
I understand that the information I give on this application both verbally and in writing will be checked. I agree to help do that and to let SoonerCare get needed information from government agencies, employers, medical providers and other sources.
I know that our Social Security numbers will be given to other government agencies to get information needed to prove eligibility.
I know I am required to help the Oklahoma Department of Human Services (OKDHS) or the Oklahoma Health Care Authority (OHCA) to identify and locate those absent parents who might be liable for the costs of medical care to me or others in my family receiving SoonerCare.
I give permission for SoonerCare to: (1) collect payments from anyone who is supposed to pay for medical care, (2) share necessary medical information with any insurance company, person or entity who is responsible for paying the bill, and (3) inspect any of my medical records to determine the compensability of claims for services. I also give permission to any of my medical providers or home care providers to give information to the OKDHS or the OHCA to make payment or overpayment decisions.
I agree to tell SoonerCare within 10 days if there are any changes in our income, the people who live in our home, where we live or get our mail, and/or our health insurance.
I know that I can ask for a fair hearing if I think the decision made on my case is unfair, incorrect or made too late.
I also know that my application for SoonerCare cannot be denied because of race, color, sex, age, disability, religion, nationality or political belief.
13.ASSIGNMENT: I do hereby transfer, assign and authorize payment to the Oklaho- ma Health Care Authority (OHCA) all claims I have or may have against health insur- ance or liability insurance companies, or other third parties. This covers all payments for medical services made by OHCA.
Yes No
This Application will be denied if you check NO to this question.
14. Your Signature______________________________ Date _____________
For ofice use only Date received __________________________
ELIGIBLE Yes No
Signature _____________________________
Date _________________________________
OKHCA Revised |
Pg 4 |