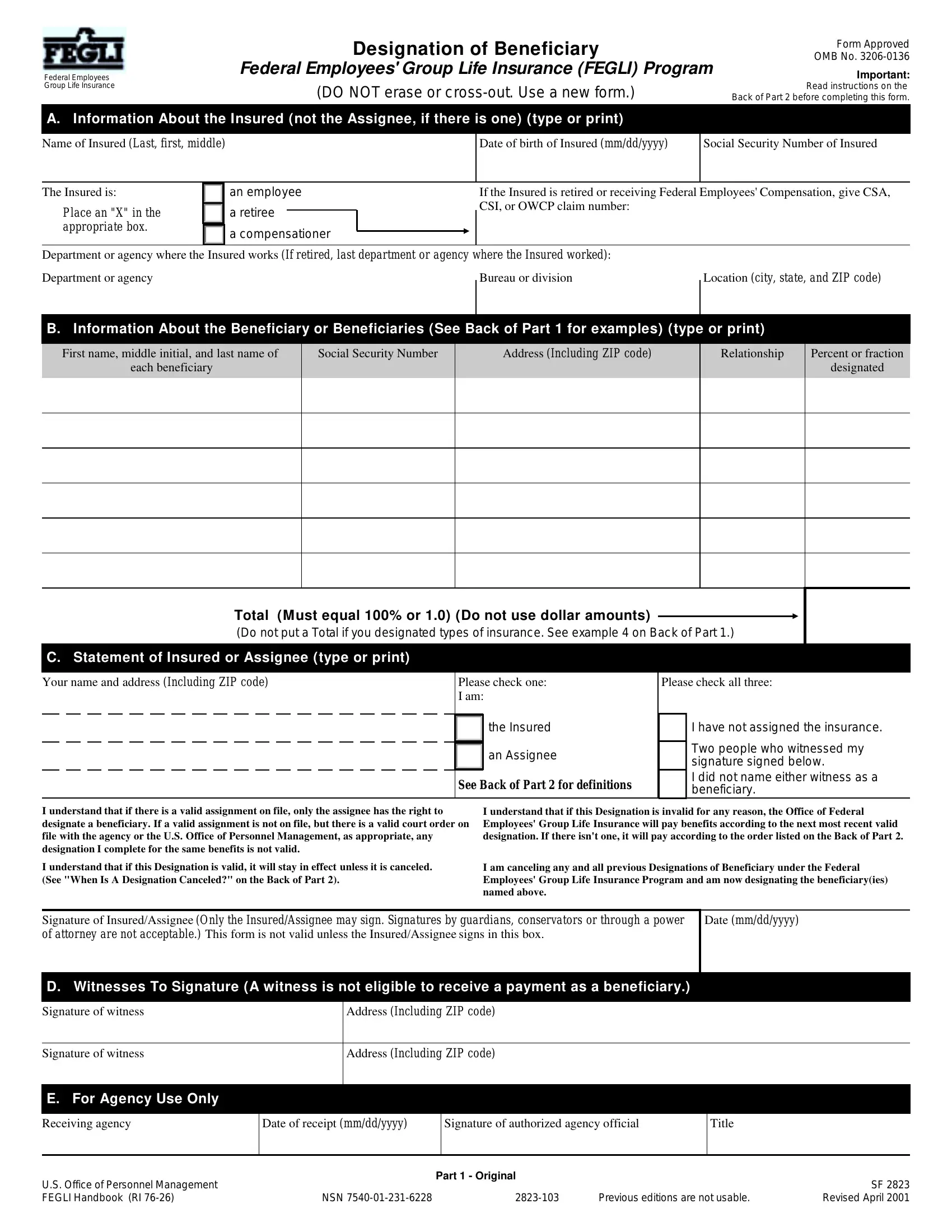
Life is filled with uncertainties, and planning for the future is a step many take to ensure peace of mind for themselves and their loved ones. For federal employees, one such planning tool is the OMB 3206-0136 form, officially known as the Federal Employees' Group Life Insurance (FEGLI) Designation of Beneficiary form. This form plays a critical role in determining how the benefits of the FEGLI Program will be distributed upon the insured's death. It requires detailed information about the insured, including their name, date of birth, social security number, and employment details, along with comprehensive data on the beneficiary or beneficiaries designated to receive the life insurance proceeds. Furthermore, it outlines a clear process for insured individuals or assignees to cancel or change a beneficiary designation, emphasizes the importance of witnesses who cannot benefit from the policy, and details the procedure for agency use. The instructions provided on the form ensure clarity on its completion and underline the importance of keeping beneficiary designations up to date, signifying the insured's intent and possibly reflecting changes in personal circumstances, such as marriage, divorce, or the birth of a child. This form isn't just paperwork; it's a critical step in securing the well-being of those we care about the most, making its proper completion and submission a priority for every federal employee enrolled in FEGLI.
| Question | Answer |
|---|---|
| Form Name | Omb Form 3206 0136 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | OPM, OFEGLI, form omb 3208, omb 3208 |