
or immunization can be completed online easily. Just try FormsPal PDF editing tool to complete the task in a timely fashion. The editor is continually improved by our staff, acquiring cool functions and turning out to be better. Here's what you will have to do to start:
Step 1: Click on the "Get Form" button at the top of this page to open our PDF editor.
Step 2: With the help of this state-of-the-art PDF editor, you're able to do more than merely fill in blank form fields. Express yourself and make your docs seem great with customized text added in, or modify the file's original input to excellence - all that accompanied by the capability to insert almost any photos and sign the file off.
This PDF will require particular data to be filled out, therefore you must take the time to type in what is requested:
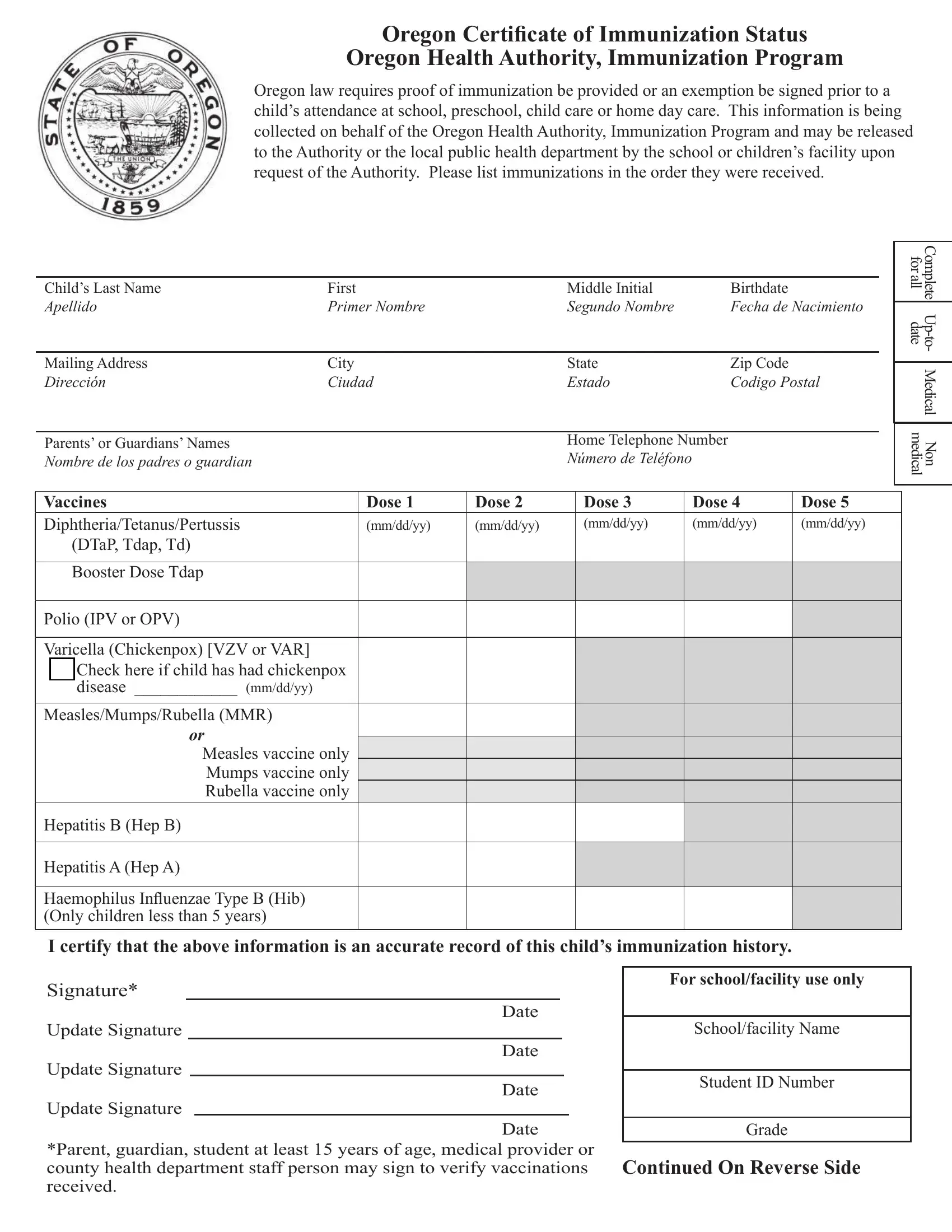
1. The or immunization requires specific information to be entered. Be sure the next blanks are filled out:
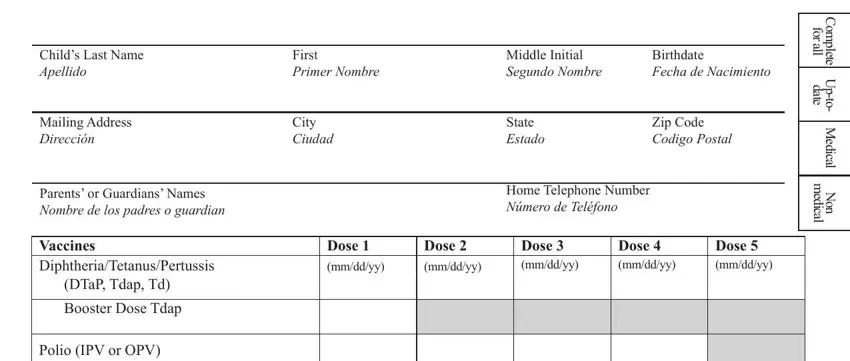
2. Once your current task is complete, take the next step – fill out all of these fields - Varicella Chickenpox VZV or VAR, o Check here if child has had, disease mmddyy, MeaslesMumpsRubella MMR, Measles vaccine only Mumps vaccine, Hepatitis B Hep B, Hepatitis A Hep A, Haemophilus In uenzae Type B Hib, I certify that the above, Signature, Update Signature, Update Signature, Date, Date, and For schoolfacility use only with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
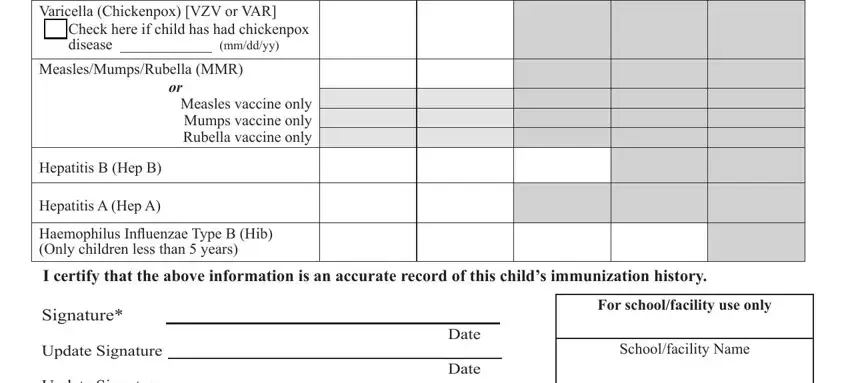
3. The following portion is mostly about Update Signature, Update Signature, Date, Date, Student ID Number, Grade, Parent guardian student at least, and Continued On Reverse Side - complete every one of these empty form fields.

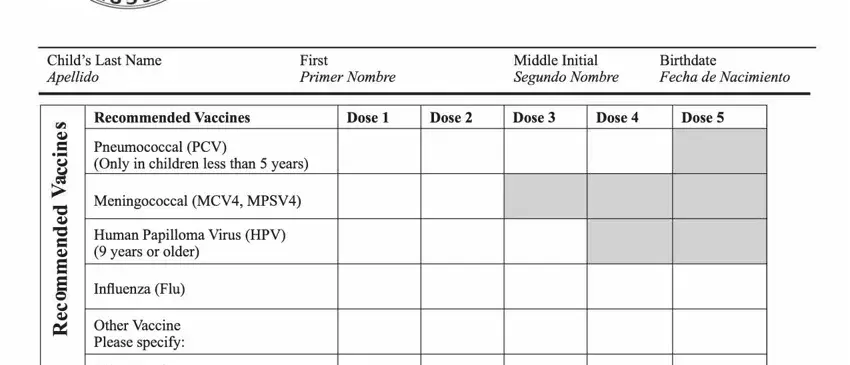
4. This next section requires some additional information. Ensure you complete all the necessary fields - Childs Last Name Apellido, First Primer Nombre, Middle Initial Segundo Nombre, Birthdate Fecha de Nacimiento, Only in children less than years, Recommended Vaccines, Pneumococcal PCV e e, Influenza Flu, CS CS, Human Papilloma Virus HPV years, Meningococcal MCV MPSV, Other Vaccine Please specify Other, Dose, Dose, and Dose - to proceed further in your process!
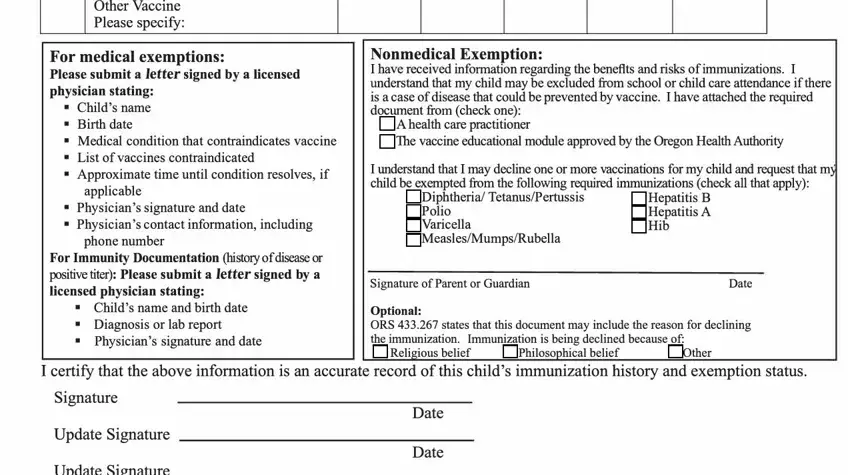
5. The last section to finish this PDF form is essential. You must fill out the appropriate blanks, consisting of Other Vaccine Please specify Other, For medical exemptions Please, applicable, Physicians signature and date, phone number, For Immunity Documentation history, Childs name and birth date, Nonmedical Exemption I have, A health care practitioner The, I understand that I may decline, Diphtheria TetanusPertussis Polio, Hepatitis B Hepatitis A Hib, Signature of Parent or Guardian, Date, and Optional ORS states that this, prior to submitting. Neglecting to do it may give you an unfinished and possibly invalid document!
Always be really attentive when completing applicable and I understand that I may decline, since this is where many people make a few mistakes.
Step 3: Before submitting this file, you should make sure that all form fields have been filled out as intended. The moment you think it is all fine, click on “Done." Join us right now and instantly get access to or immunization, prepared for downloading. All alterations you make are saved , so that you can customize the document later on as required. Here at FormsPal.com, we do everything we can to ensure that all of your details are kept protected.