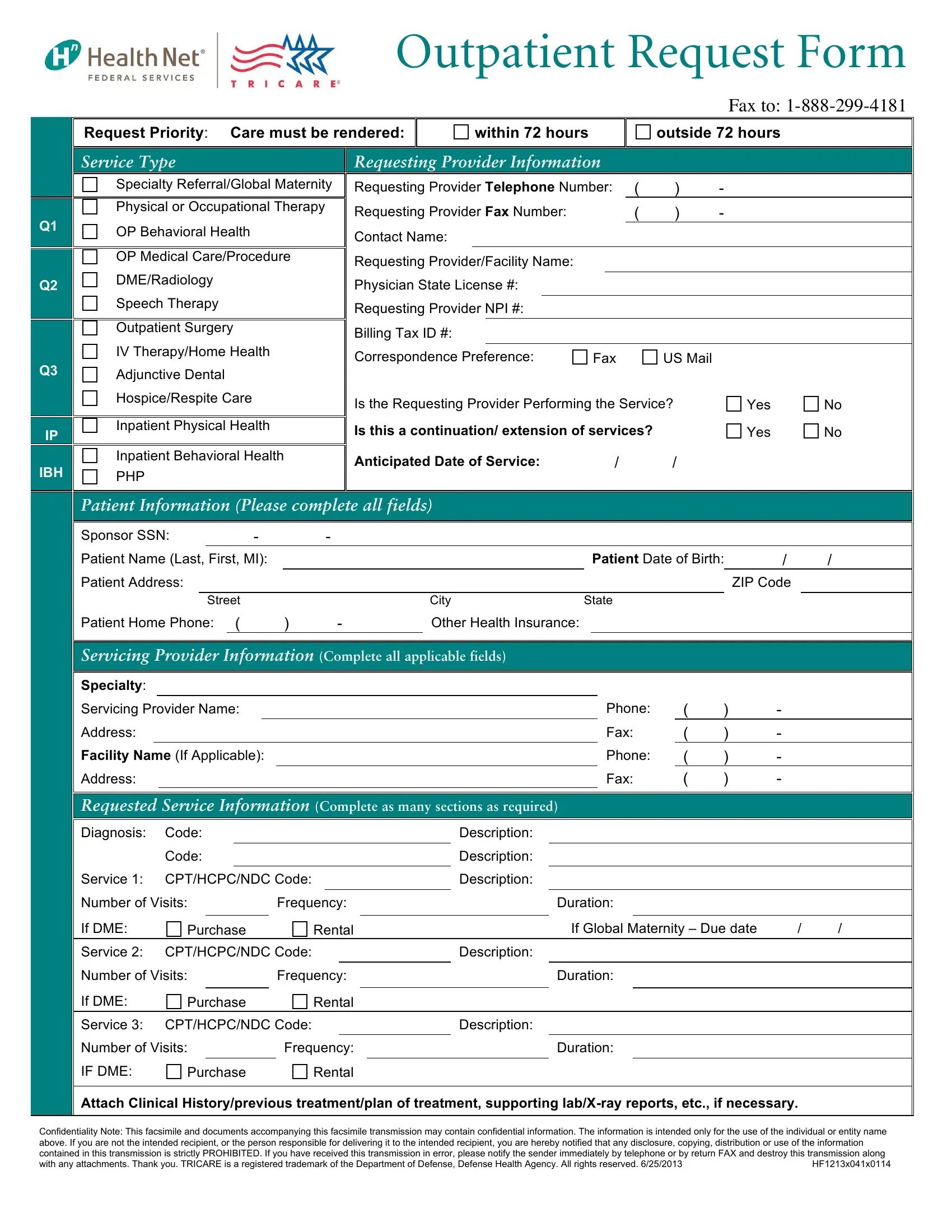
In the realm of healthcare management, the Outpatient Request Form serves as a critical tool in facilitating a range of services vital to patient care. This form, which must be faxed to a specific number, delineates the requirements and procedures needed for patients seeking outpatient services. Priority is given to the urgency of care, distinguishing between care needed within 72 hours and that which falls outside this immediate timeframe. The form is comprehensive, covering a range of service types such as specialty referrals, physical or occupational therapy, outpatient surgery, and more, each with its own section for detailed information including diagnostics and anticipated service needs. It also addresses equipment needs, from diagnostics to durable medical equipment (DME) and outlines the necessity for additional services like hospice or home health. Importantly, the form requests detailed provider information, ensuring that the person requesting the service is clearly identified by their license number, contact details, and preferences for correspondence. It even specifies whether the requesting provider will perform the service, highlighting the importance of continuity and coordination of care. Patient information is meticulously requested, ensuring a comprehensive understanding of their healthcare coverage and any other health insurance they might have. For services rendered, detailed information about the diagnosis, the specific services required, and their anticipated frequency and duration must be meticulously completed. The form underscores the importance of attaching relevant clinical history and diagnostic reports to support the request, emphasizing the role of thorough documentation in delivering effective outpatient care. Additionally, the inclusion of a confidentiality note underscores the sensitive nature of the information handled, aligning with best practices in patient privacy and security. With the stipulation that misuse or unauthorized disclosure of the information is strictly prohibited, the form ensures compliance with regulatory standards, safeguarding both provider and patient interests.
| Question | Answer |
|---|---|
| Form Name | Outpatient Request Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | tricare outpatient request form, health net outpatient request form, outpatient request form health, hnfs request form online |
