
With the online editor for PDFs by FormsPal, it is possible to fill in or alter pa 162 rm here and now. The editor is continually improved by us, acquiring handy features and growing to be more versatile. To get the process started, take these easy steps:
Step 1: Click on the orange "Get Form" button above. It will open our pdf editor so that you could begin completing your form.
Step 2: When you access the PDF editor, you will get the document prepared to be filled in. Aside from filling in different fields, you might also perform several other actions with the form, namely adding custom words, modifying the original textual content, inserting graphics, signing the form, and more.
This form requires specific info to be filled out, therefore make sure to take the time to enter exactly what is expected:
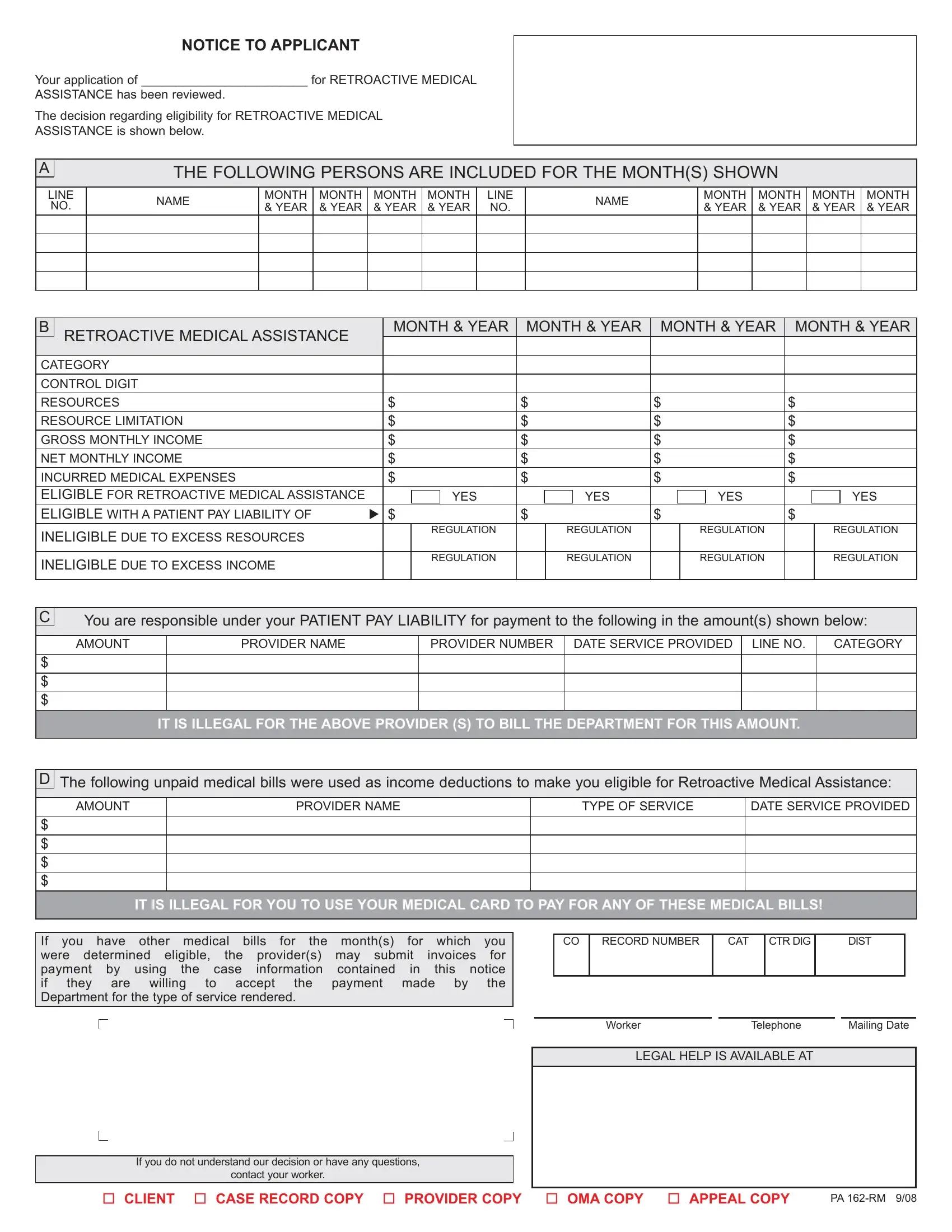
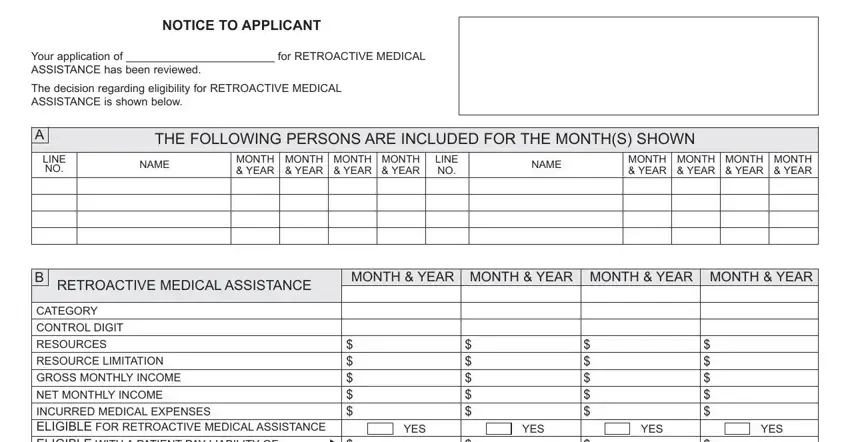
1. You have to complete the pa 162 rm properly, so take care when filling out the parts that contain these specific fields:
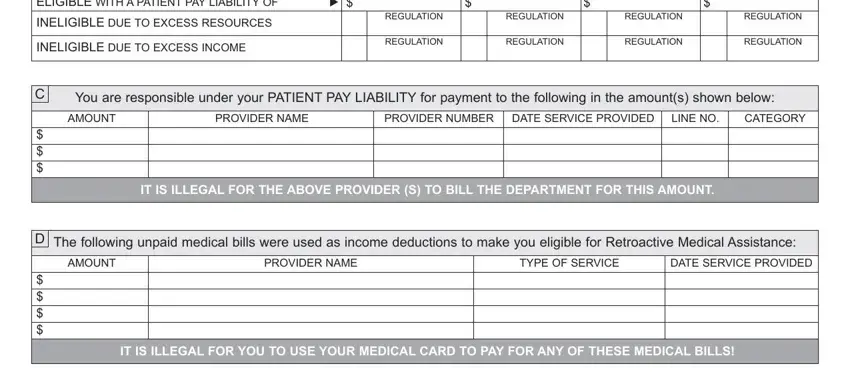
2. After filling in this part, head on to the next stage and fill in the essential details in all these blank fields - INCURRED MEDICAL EXPENSES ELIGIBLE, INELIGIBLE DUE TO EXCESS RESOURCES, INELIGIBLE DUE TO EXCESS INCOME, REGULATION, REGULATION, REGULATION, REGULATION, REGULATION, REGULATION, REGULATION, REGULATION, You are responsible under your, AMOUNT, PROVIDER NAME, and PROVIDER NUMBER.
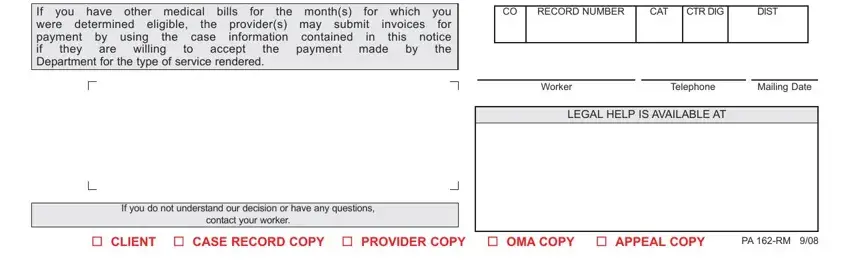
3. This subsequent segment is considered quite straightforward, If you have other medical bills, are willing, the case, accept, they, invoices, for which you for this notice the, the, payment made, for, the months, the providers may submit, information contained, RECORD NUMBER, and CAT - all of these form fields has to be filled in here.
Lots of people often make mistakes when completing invoices in this section. Ensure that you read twice whatever you type in here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - PLEASE CHECK THE BOX NEXT TO THE, will be on the phone from the CAO, PLEASE CHECK BELOW IF YOU NEED, I WANT TO REQUEST A HEARING BECAUSE, DATE, CLIENT REPRESENTATIVE SIGNATURE, TELEPHONE, DATE, CLIENT SIGNATURE, TELEPHONE, CLIENT ADDRESS, and HEARING LOCATIONS - to proceed further in your process!
Step 3: Confirm that your information is correct and then press "Done" to complete the project. Make a 7-day free trial option at FormsPal and get instant access to pa 162 rm - download or modify inside your FormsPal cabinet. FormsPal guarantees your data confidentiality via a secure method that never saves or distributes any sort of private information used. Feel safe knowing your paperwork are kept safe any time you use our editor!