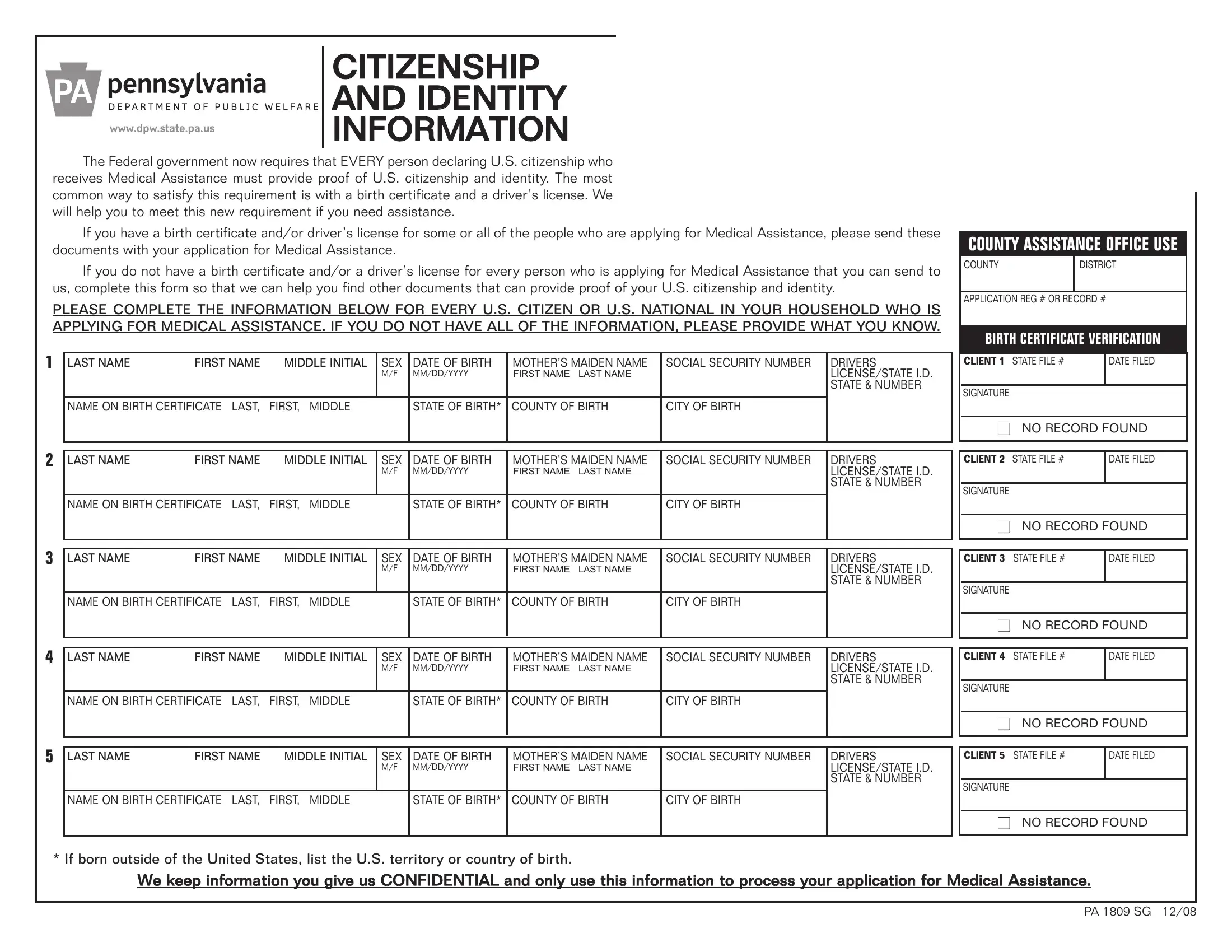
In light of the federal government's updated requirements, individuals declaring U.S. citizenship and applying for Medical Assistance need to provide definitive proof of both citizenship and identity. A significant step in complying with these regulations involves the submission or procurement of specific documents, primarily a birth certificate and a driver’s license. The PA 1809 SG form serves as a crucial tool in this process. It's designed to gather essential information about each U.S. citizen or national within a household applying for Medical Assistance. This form asks for detailed personal data, including names, sex, birthdates, social security numbers, and information about birth certificates and state identification. It provides a structured way for applicants who may not readily have all necessary documents to seek assistance in meeting these requirements. Moreover, for households lacking immediate access to such documents for all members, it outlines a procedure for identifying alternative documents that can prove citizenship and identity. Confidentiality of the information provided is a primary commitment, ensuring that the collected data is solely used for processing the Medical Assistance application. By using this form, individuals find a clearer pathway to compliance, reinforcing the overarching goal of maintaining the integrity of the application process while also receiving the required assistance.
| Question | Answer |
|---|---|
| Form Name | Pa 1809 Sg Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | what is form pa 1809, 1809 pa form, sg pa citizen, pennsylvania 1809 |
CITIZENSHIP
AND IDENTITY
INFORMATION
The Federal government now requires that EVERY person declaring U.S. citizenship who receives Medical Assistance must provide proof of U.S. citizenship and identity. The most common way to satisfy this requirement is with a birth certificate and a driver’s license. We will help you to meet this new requirement if you need assistance.
If you have a birth certificate and/or driver’s license for some or all of the people who are applying for Medical Assistance, please send these documents with your application for Medical Assistance.
If you do not have a birth certificate and/or a driver’s license for every person who is applying for Medical Assistance that you can send to us, complete this form so that we can help you find other documents that can provide proof of your U.S. citizenship and identity.
PLEASE COMPLETE THE INFORMATION BELOW FOR EVERY U.S. CITIZEN OR U.S. NATIONAL IN YOUR HOUSEHOLD WHO IS APPLYING FOR MEDICAL ASSISTANCE. IF YOU DO NOT HAVE ALL OF THE INFORMATION, PLEASE PROVIDE WHAT YOU KNOW.
1 |
LAST NAME |
FIRST NAME |
MIDDLE INITIAL |
SEX |
DATE OF BIRTH |
MOTHER’S MAIDEN NAME |
SOCIAL SECURITY NUMBER |
DRIVERS |
|
|
|
|
M/F |
MM/DD/YYYY |
FIRSTNAME LASTNAME |
|
LICENSE/STATE I.D. |
|
|
|
|
|
|
|
|
STATE & NUMBER |
|
|
|
|
|
|
|
|
|
|
NAME ON BIRTH CERTIFICATE LAST, |
FIRST, MIDDLE |
|
STATE OF BIRTH* |
COUNTY OF BIRTH |
CITY OF BIRTH |
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
FIRST NAME |
MIDDLE INITIAL |
SEX |
DATE OF BIRTH |
MOTHER’S MAIDEN NAME |
SOCIAL SECURITY NUMBER |
DRIVERS |
|
|
|
|
|
M/F |
MM/DD/YYYY |
FIRSTNAME LASTNAME |
|
LICENSE/STATE I.D. |
|
|
|
|
|
|
|
|
STATE & NUMBER |
|
|
|
|
|
|
|
|
|
|
NAME ON BIRTH CERTIFICATE LAST, |
FIRST, MIDDLE |
|
STATE OF BIRTH* |
COUNTY OF BIRTH |
CITY OF BIRTH |
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
FIRST NAME |
MIDDLE INITIAL |
SEX |
DATE OF BIRTH |
MOTHER’S MAIDEN NAME |
SOCIAL SECURITY NUMBER |
DRIVERS |
|
|
|
|
|
M/F |
MM/DD/YYYY |
FIRSTNAME LASTNAME |
|
LICENSE/STATE I.D. |
|
|
|
|
|
|
|
|
STATE & NUMBER |
|
|
|
|
|
|
|
|
|
|
NAME ON BIRTH CERTIFICATE LAST, |
FIRST, MIDDLE |
|
STATE OF BIRTH* |
COUNTY OF BIRTH |
CITY OF BIRTH |
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
FIRST NAME |
MIDDLE INITIAL |
SEX |
DATE OF BIRTH |
MOTHER’S MAIDEN NAME |
SOCIAL SECURITY NUMBER |
DRIVERS |
|
|
|
|
|
M/F |
MM/DD/YYYY |
FIRSTNAME LASTNAME |
|
LICENSE/STATE I.D. |
|
|
|
|
|
|
|
|
STATE & NUMBER |
|
|
|
|
|
|
|
|
|
|
NAME ON BIRTH CERTIFICATE LAST, |
FIRST, MIDDLE |
|
STATE OF BIRTH* |
COUNTY OF BIRTH |
CITY OF BIRTH |
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
FIRST NAME |
MIDDLE INITIAL |
SEX |
DATE OF BIRTH |
MOTHER’S MAIDEN NAME |
SOCIAL SECURITY NUMBER |
DRIVERS |
|
|
|
|
|
M/F |
MM/DD/YYYY |
FIRSTNAME LASTNAME |
|
LICENSE/STATE I.D. |
|
|
|
|
|
|
|
|
STATE & NUMBER |
|
|
|
|
|
|
|
|
|
|
NAME ON BIRTH CERTIFICATE LAST, |
FIRST, MIDDLE |
|
STATE OF BIRTH* |
COUNTY OF BIRTH |
CITY OF BIRTH |
|
|
|
|
|
|
|
|
|
|
|
COUNTY ASSISTANCE OFFICE USE
COUNTY |
DISTRICT |
|
|
APPLICATION REG # OR RECORD #
BIRTH CERTIFICATE VERIFICATION
|
CLIENT 1 STATE FILE # |
DATE FILED |
|
|
|
|
SIGNATURE |
|
■NO RECORD FOUND
|
CLIENT 2 STATE FILE # |
DATE FILED |
|
|
|
SIGNATURE
■NO RECORD FOUND
|
CLIENT 3 STATE FILE # |
DATE FILED |
|
|
|
SIGNATURE
■NO RECORD FOUND
|
CLIENT 4 STATE FILE # |
DATE FILED |
|
|
|
SIGNATURE
■NO RECORD FOUND
|
CLIENT 5 STATE FILE # |
DATE FILED |
|
|
|
SIGNATURE
■NO RECORD FOUND
* If born outside of the United States, list the U.S. territory or country of birth.
We keep information you give us CONFIDENTIAL and only use this information to process your application for Medical Assistance.
PA 1809 SG 12/08