Ensuring civil rights compliance is a pivotal aspect for many organizations and facilities within Pennsylvania, necessitating a thorough understanding of the Pa Civil Rights Compliance form. This form is a comprehensive questionnaire designed to affirm an entity's adherence to non-discrimination policies in both service provision and employment practices. It requires the submission of detailed information including the facility's legal name, addresses, contact information of responsible officials, as well as the facility's type, ranging from multi-facility systems to single-site operations. The heart of the compliance form lies within its probing inquiries into how organizations develop, disseminate, and enforce non-discrimination policies. This encompasses methods of reaching out to non-English speakers, ensuring accessibility for individuals with disabilities, and outlining procedures for raising and addressing complaints of discrimination. By delving into such depths, the form serves as both a tool for self-audit by organizations and a mechanism for state oversight, ensuring that services and employment opportunities within the state of Pennsylvania are offered with equity, dignity, and respect for all individuals, regardless of race, color, religious creed, disability, ancestry, national origin, age, or sex.
| Question | Answer |
|---|---|
| Form Name | Pa Civil Rights Compliance Form |
| Form Length | 10 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 30 sec |
| Other names | compliance civil rights pa, civil right compliance, pa civil rights compliance, pennsylvania civil rights survey |

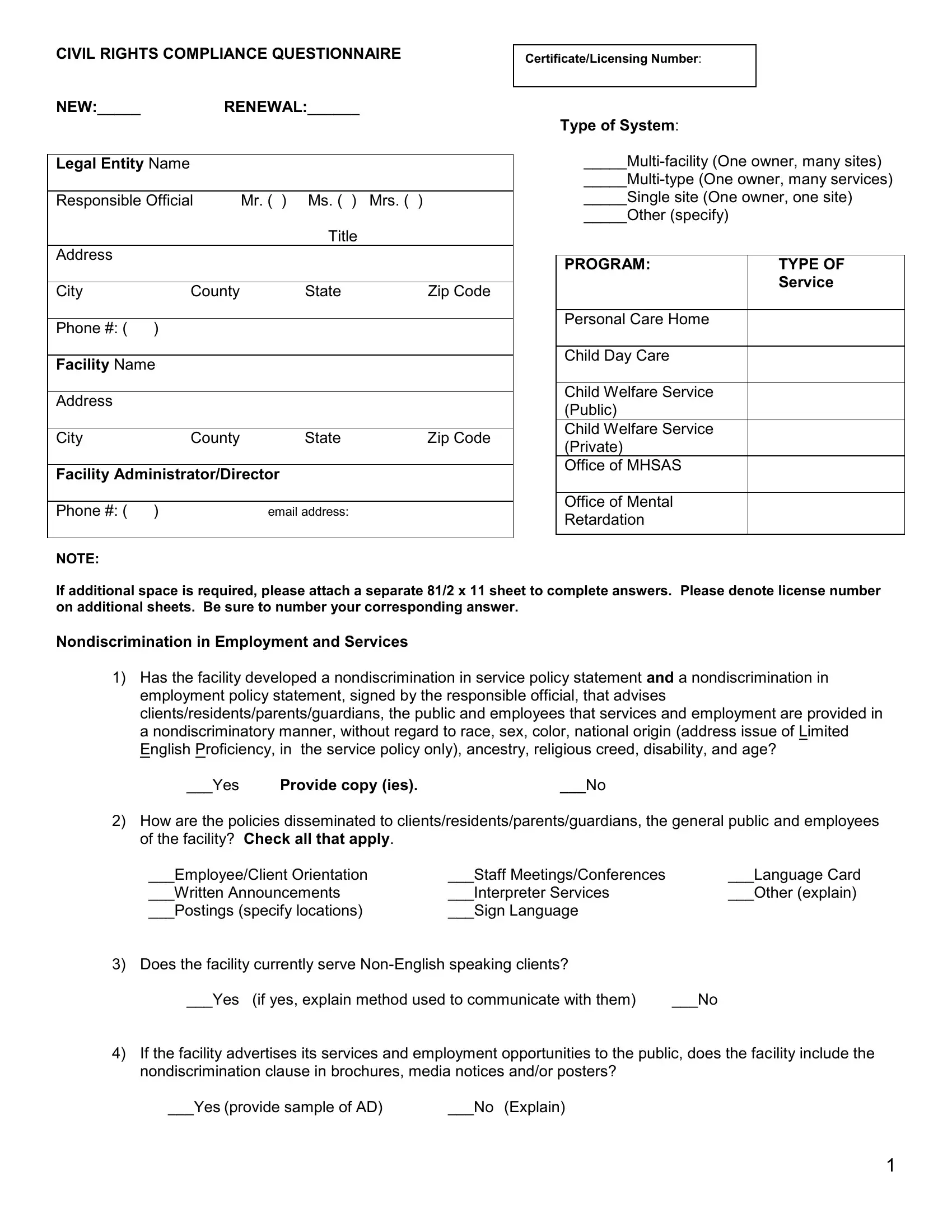
CIVIL RIGHTS COMPLIANCE QUESTIONNAIRE
Certificate/Licensing Number:
NEW:_____ |
RENEWAL:______ |
|
|
|
|
|
|
Legal Entity Name |
|
|
|
|
|
|
|
Responsible Official |
Mr. ( ) Ms. ( ) |
Mrs. ( ) |
|
|
|
Title |
|
Address |
|
|
|
|
|
|
|
City |
County |
State |
Zip Code |
|
|
|
|
Phone #: ( |
) |
|
|
|
|
|
|
Facility Name |
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
City |
County |
State |
Zip Code |
|
|
||
Facility Administrator/Director |
|
||
|
|
|
|
Phone #: ( |
) |
email address: |
|
|
|
|
|
NOTE:
Type of System:
_____Single site (One owner, one site)
_____Other (specify)
PROGRAM: |
TYPE OF |
|
Service |
|
|
Personal Care Home |
|
|
|
Child Day Care |
|
|
|
Child Welfare Service |
|
(Public) |
|
Child Welfare Service |
|
(Private) |
|
Office of MHSAS |
|
|
|
Office of Mental |
|
Retardation |
|
|
|
If additional space is required, please attach a separate 81/2 x 11 sheet to complete answers. Please denote license number on additional sheets. Be sure to number your corresponding answer.
Nondiscrimination in Employment and Services
1)Has the facility developed a nondiscrimination in service policy statement and a nondiscrimination in employment policy statement, signed by the responsible official, that advises clients/residents/parents/guardians, the public and employees that services and employment are provided in a nondiscriminatory manner, without regard to race, sex, color, national origin (address issue of Limited English Proficiency, in the service policy only), ancestry, religious creed, disability, and age?
___Yes |
Provide copy (ies). |
___No |
2)How are the policies disseminated to clients/residents/parents/guardians, the general public and employees of the facility? Check all that apply.
___Employee/Client Orientation |
___Staff Meetings/Conferences |
___Language Card |
___Written Announcements |
___Interpreter Services |
___Other (explain) |
___Postings (specify locations) |
___Sign Language |
|
3) Does the facility currently serve
___Yes (if yes, explain method used to communicate with them) |
___No |
4)If the facility advertises its services and employment opportunities to the public, does the facility include the nondiscrimination clause in brochures, media notices and/or posters?
___Yes (provide sample of AD) |
___No (Explain) |
1
5)Are clients, residents, parents/guardians informed that complaints of discrimination may be filed with the U.S. Department of Health and Human Services’ Office of Civil Rights, the DPW Bureau of Equal Opportunity
(BEO) and/or the Pennsylvania Human Relations Commission (PHRC)?
___Yes (Explain how the content is disseminated) |
___ No (Please Explain) |
6)Has information been provided to all staff regarding their rights to file complaints of employment discrimination based on Title VII of the Civil Rights Act of 1964, Section 504 of the Rehabilitation Act of 1973, the Age Discrimination Act of 1975, and/or the Pennsylvania Human Relations Act of 1955, as amended with the PHRC or Equal Employment Opportunity Commission (EEOC)?
___ Yes (Please specify method used to inform staff) |
____ No |
|
___Employee orientation |
___Staff meetings/conferences |
|
___Written announcements |
___Other (explain) |
|
7)Are restrooms, drinking fountains (e.g. human needs facilities) accessible to disabled clients/ residents/ parents/ employees/ visitors?
___ Yes |
____ No ( Explain). |
8)How are minorities and persons with disabilities or with Limited English Proficiency integrated into programs and activities?
Please Explain
9)What methods are employed to make services accessible to those who may have mobility or sensory
impairments? CHECK ALL THAT APPLY
___Building modifications |
___Program relocation within the structure |
___Other (specify) |
___Auxiliary aids |
___Program relocation to another structure |
|
10)Does the facility’s nondiscrimination policy state that a reasonable accommodation will be provided for employees/clients with a disability (e.g. hearing, speech, vision, mobility impairments)? Have any been
granted/denied in the past 12 months? |
Please Explain. |
11)Within the last 12 months, have any complaints of discrimination been filed with PHRC or EEOC? List each and explain in detail the current status.
Governing Board – If Applicable
1)What policy or criteria is used to select Board members?
2)If the facility has a Board, describe methods and materials used to orient the Board to its Civil Rights compliance requirements.
The information submitted is, to the best of my knowledge, true and we intend to be bound by it.
___________________________ |
_______________________________ |
____________ |
Responsible Official Name (Print) |
Signature |
Date |
NOTE: An unannounced facility
2
Attachment I
License Number__________
Facility___________________________
Language of Current Limited English Proficient Clients
Current Clients Served
Total
Black |
|
Hispanic |
|
White |
|
Native |
Asian/Pacific |
OTHERS |
|||||||
|
|
|
|
|
|
|
|
|
American |
Islander |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
F |
M |
|
F |
M |
|
F |
M |
F |
M |
|
F |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total
Total Client Admissions in the Past 12 Months
Black |
|
Hispanic |
|
White |
|
Native |
Asian/Pacific |
OTHERS |
||||||||
|
|
|
|
|
|
|
|
|
American |
Islander |
|
|
|
|||
M |
|
F |
M |
|
F |
M |
|
F |
M |
|
F |
M |
|
F |
|
|
|
|
|
|
|
M |
F |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spanish
Chinese (Specify Dialects)
Russian
Cambodian
Vietnamese |
Other |
|
(Specify Language) |
|
|
Board Composition – Should be reflective of community and client base
Board Member |
Race |
Sex |
Disability |
Group Represented |
Date Term |
(Names may be omitted) |
* |
|
|
|
Expires |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Race Code: B = Black, H = Hispanic, W = White, NA = Native American, A/PI = Asian/Pacific Islander
Employment Information – Current Employees
Job Title/ |
Total Staff |
Black |
|
Hispanic |
White |
||||
Classification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
M |
|
F |
M |
F |
M |
F |
|
|
|
|
|
|
|
|
|
|
Native
American
MF
Asian/ |
|
|
|
Pacific |
Others |
||
Islander |
|
|
|
M |
F |
M |
F |
|
|
|
|
3
For recruitment purposes: Minority/Women/Disabled Groups Contacted
Current Client Information: Please fill in the number of clients served below.
Name of Organization
Contacted
Group Represented
(Minority/Women/Disabled)
Purpose of
Contact
Method of
Contact
Phone/Mail
Date of Contact
Name of Person
Contacted
Workforce should show parity in keeping with community/client base served.
Current Employees Enrolled in Training Programs – listing of any courses offered over the past 12 months
|
|
|
|
|
|
|
|
|
Native |
Asian/ |
|
|
||
Course Title |
Total |
Black |
Hispanic |
White |
American |
Pacific |
Others |
|||||||
|
|
|
|
|
|
|
|
|
|
|
Islander |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Completed by MH/MR ONLY
|
|
|
|
|
|
|
|
|
|
|
Native |
|
Asian/ |
|
|
||
|
Total |
Black |
Hispanic |
|
White |
American |
|
Pacific |
Others |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Islander |
|
|
||
Service Offered under |
M |
F |
M |
F |
M |
F |
M |
|
F |
M |
|
F |
M |
|
F |
M |
F |
license number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REV (10/08)
4
COMMONWEALTH OF PENNSYLVANIA (►Use Private Letterhead)
SAMPLE # 1 - CENTRAL REGION
SUBJECT: Nondiscrimination Policy Statement
Equal Employment Opportunity
TO: Staff
FROM: (►Insert Director’s Name and Signature)
An open and equitable personnel systems will be established and maintained. Personnel policies, procedures and practices will be designed to prohibit discrimination on the basis of race, color, religious creed, disability, ancestry, national origin (including limited English proficiency), age, or sex.
Employment opportunities shall be provided for applicants with disabilities and reasonable accommodation(s) shall be made to meet the physical or mental limitations of qualified applicants or employees.
Any employee who believes they have been discriminated against, may file a complaint of discrimination with any of the following.
(►Insert Provider/Facility’s Name)
(►Insert Address)
Department of Public Welfare |
PA Human Relations Commission |
Bureau of Equal Opportunity |
Harrisburg Regional Office |
Room 223, Health & Welfare Building |
Riverfront Office Center |
625 Forster Street |
1101 S. Front St., 5th Floor |
Harrisburg, PA 17120 |
Harrisburg, PA 17104 |
U.S. Dpt. of Health & Human Services
Office for Civil Rights
Suite 372, Public Ledger Bldg.
150 South Independence Mall West
Philadelphia, PA
5
COMMONWEALTH OF PENNSYLVANIA (►Use Private Letterhead)
SAMPLE # 2 – CENTRAL REGION
SUBJECT: Nondiscrimination in Services
TO: Patients/Clients/Residents/Parents
(►Insert one of the above, as applicable)
FROM: (►Insert Director’s Name and Signature)
Admissions, the provisions of services, and referrals of clients shall be made without regard to race, color, religious creed, disability, ancestry, national origin (including limited English proficiency), age, or sex.
Program services shall be made accessible to eligible persons with disabilities through the most practical and economically feasible methods available. These methods include, but are not limited to, equipment redesign, the provision of aides, and the use of alternative service delivery locations. Structural modifications shall be considered only as a last resort among available methods.
Any individual/client/patient/student (and /or their guardian) who believes they have been discriminated against, may file a complaint of discrimination with:
(►Insert Provider/Facility Name)
(►Insert Address)
Department of Public Welfare |
PA Human Relations Commission |
Bureau of Equal Opportunity |
Harrisburg Regional Office |
Room 223, Health & Welfare Building |
Riverfront Office Center |
625 Forster Street |
1101 S. Front St., 5th Floor |
Harrisburg, PA 17120 |
Harrisburg, PA 17104 |
U.S. Dpt. of Health & Human Services
Office for Civil Rights
Suite 372, Public Ledger Bldg.
150 South Independence Mall West
Philadelphia, PA
6
COMMONWEALTH OF PENNSYLVANIA (►Use Private Letterhead)
SAMPLE # 1 – SOUTHEAST REIGON
SUBJECT: Nondiscrimination Policy Statement
Equal Employment Opportunity
TO: Staff
FROM: (►Insert Director’s Name and Signature)
An open and equitable personnel systems will be established and maintained. Personnel policies, procedures and practices will be designed to prohibit discrimination on the basis of race, color, religious creed, disability, ancestry, national origin (including limited English proficiency), age, or sex.
Employment opportunities shall be provided for applicants with disabilities and reasonable accommodation(s) shall be made to meet the physical or mental limitations of qualified applicants or employees.
Any employee who believes they have been discriminated against, may file a complaint of discrimination with any of the following.
(►Insert Provider/Facility’s Name)
(►Insert Address)
Department of Public Welfare |
PA Human Relations Commission |
Bureau of Equal Opportunity |
110 North 8th Street |
Room 223, Health & Welfare Building |
Suite 501 |
625 Forster Street |
Philadelphia, PA 19107 |
Harrisburg, PA 17120 |
|
U.S. Dpt. of Health & Human Services |
Commonwealth of Pennsylvania |
Office for Civil Rights |
DPW/ Bureau of Equal Opportunity |
Suite 372, Public Ledger Bldg. |
Southeast Regional Office |
150 South Independence Mall West |
801 Market Street, Suite 5034 |
Philadelphia, PA |
Philadelphia, PA 19107 |
7
COMMONWEALTH OF PENNSYLVANIA (►Use Private Letterhead)
SAMPLE # 2 – SOUTHEAST REGION
SUBJECT: Nondiscrimination in Services
TO: Patients/Clients/Residents/Parents
(►Insert one of the above, as applicable)
FROM: (►Insert Director’s Name and Signature)
Admissions, the provisions of services, and referrals of clients shall be made without regard to race, color, religious creed, disability, ancestry, national origin (including limited English proficiency), age, or sex.
Program services shall be made accessible to eligible persons with disabilities through the most practical and economically feasible methods available. These methods include, but are not limited to, equipment redesign, the provision of aides, and the use of alternative service delivery locations. Structural modifications shall be considered only as a last resort among available methods.
Any individual/client/patient/student (and /or their guardian) who believes they have been discriminated against, may file a complaint of discrimination with:
(►Insert Provider/Facility Name)
(►Insert Address)
Department of Public Welfare |
PA Human Relations Commission |
Bureau of Equal Opportunity |
110 North 8th Street |
Room 223, Health & Welfare Building |
Suite 501 |
625 Forster Street |
Philadelphia, PA 19107 |
Harrisburg, PA 17120 |
|
U.S. Dpt. of Health & Human Services |
Commonwealth of Pennsylvania |
Office for Civil Rights |
DPW/ Bureau of Equal Opportunity |
Suite 372, Public Ledger Bldg. |
Southeast Regional Office |
150 South Independence Mall West |
801 Market Street, Suite 5034 |
Philadelphia, PA |
Philadelphia, PA 19107 |
8
COMMONWEALTH OF PENNSYLVANIA (►Use Private Letterhead)
SAMPLE # 1 – WESTERN REGION
SUBJECT: Nondiscrimination Policy Statement
Equal Employment Opportunity
TO: Staff
FROM: (►Insert Director’s Name and Signature)
An open and equitable personnel systems will be established and maintained. Personnel policies, procedures and practices will be designed to prohibit discrimination on the basis of race, color, religious creed, disability, ancestry, national origin, age, or sex.
Employment opportunities shall be provided for applicants with disabilities and reasonable accommodation(s) shall be made to meet the physical or mental limitations of qualified applicants or employees.
Any employee who believes they have been discriminated against, may file a complaint of discrimination with any of the following.
(►Insert Provider/Facility’s Name)
(►Insert Address)
Department of Public Welfare |
PA Human Relations Commission |
Bureau of Equal Opportunity |
301 Fifth Avenue |
Room 223, Health & Welfare Building |
Suite 390, Piatt Place |
625 Forster Street |
Pittsburgh, PA 15222 |
Harrisburg, PA 17120 |
|
U. S. Department of Health and Human Services |
Department of Public Welfare |
Office for Civil Rights |
Bureau of Equal Opportunity |
Suite 372, Public Ledger Bldg. |
Western Regional Office |
150 South Independence Mall West |
301 Fifth Avenue |
Philadelphia, PA 19106 |
Suite 410, Piatt Place |
|
Pittsburgh, PA |
9
COMMONWEALTH OF PENNSYLVANIA (►Use Private Letterhead)
SAMPLE # 2 – WESTERN REGION
SUBJECT: Nondiscrimination in Services
TO: Patients/Clients/Residents/Parents
(►Insert one of the above, as applicable)
FROM:(►Insert Director’s Name and Signature)
Admissions, the provisions of services, and referrals of clients shall be made without regard to race, color, religious creed, disability, ancestry, national origin (including limited English proficiency), age, or sex.
Program services shall be made accessible to eligible persons with disabilities through the most practical and economically feasible methods available. These methods include, but are not limited to, equipment redesign, the provision of aides, and the use of alternative service delivery locations. Structural modifications shall be considered only as a last resort among available methods.
Any individual/client/patient/student (and /or their guardian) who believes they have been discriminated against, may file a complaint of discrimination with:
(►Insert Provider/Facility Name)
(►Insert Address)
Department of Public Welfare |
PA Human Relations Commission |
Bureau of Equal Opportunity |
301 Fifth Avenue |
Room 223, Health & Welfare Building |
Suite 390, Piatt Place |
625 Forster Street |
Pittsburgh, PA 15222 |
Harrisburg, PA 17120 |
|
U. S. Department of Health and Human Services |
Department of Public Welfare |
Office for Civil Rights |
Bureau of Equal Opportunity |
Suite 372, Public Ledger Bldg. |
Western Regional Office |
150 South Independence Mall West |
301 Fifth Avenue |
Philadelphia, PA 19106 |
Suite 410, Piatt Place |
|
Pittsburgh, PA |
10