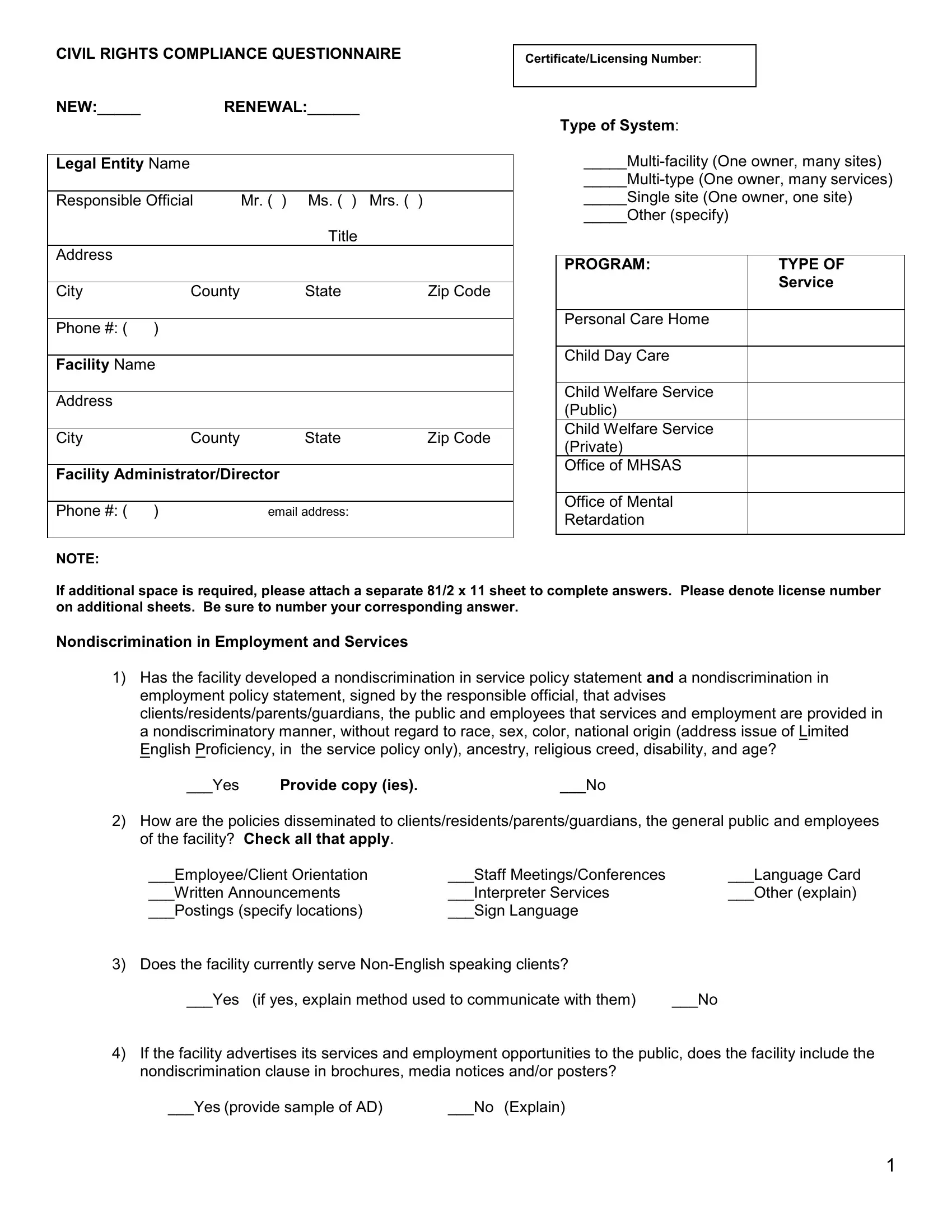
Ensuring civil rights compliance is a pivotal aspect for many organizations and facilities within Pennsylvania, necessitating a thorough understanding of the Pa Civil Rights Compliance form. This form is a comprehensive questionnaire designed to affirm an entity's adherence to non-discrimination policies in both service provision and employment practices. It requires the submission of detailed information including the facility's legal name, addresses, contact information of responsible officials, as well as the facility's type, ranging from multi-facility systems to single-site operations. The heart of the compliance form lies within its probing inquiries into how organizations develop, disseminate, and enforce non-discrimination policies. This encompasses methods of reaching out to non-English speakers, ensuring accessibility for individuals with disabilities, and outlining procedures for raising and addressing complaints of discrimination. By delving into such depths, the form serves as both a tool for self-audit by organizations and a mechanism for state oversight, ensuring that services and employment opportunities within the state of Pennsylvania are offered with equity, dignity, and respect for all individuals, regardless of race, color, religious creed, disability, ancestry, national origin, age, or sex.
| Question | Answer |
|---|---|
| Form Name | Pa Civil Rights Compliance Form |
| Form Length | 10 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 30 sec |
| Other names | compliance civil rights pa, civil right compliance, pa civil rights compliance, pennsylvania civil rights survey |