

Through the online PDF tool by FormsPal, you may fill in or modify pa form 145 here. FormsPal team is constantly working to expand the tool and enable it to be much faster for clients with its many functions. Uncover an endlessly revolutionary experience now - explore and uncover new opportunities along the way! It just takes several simple steps:
Step 1: Click on the "Get Form" button above. It's going to open up our editor so you can begin filling out your form.
Step 2: With this advanced PDF editing tool, it is easy to do more than just fill in forms. Express yourself and make your docs look high-quality with custom textual content added in, or modify the file's original content to perfection - all comes along with the capability to incorporate your own graphics and sign it off.
This document will require you to type in specific details; to guarantee correctness, please be sure to heed the tips directly below:
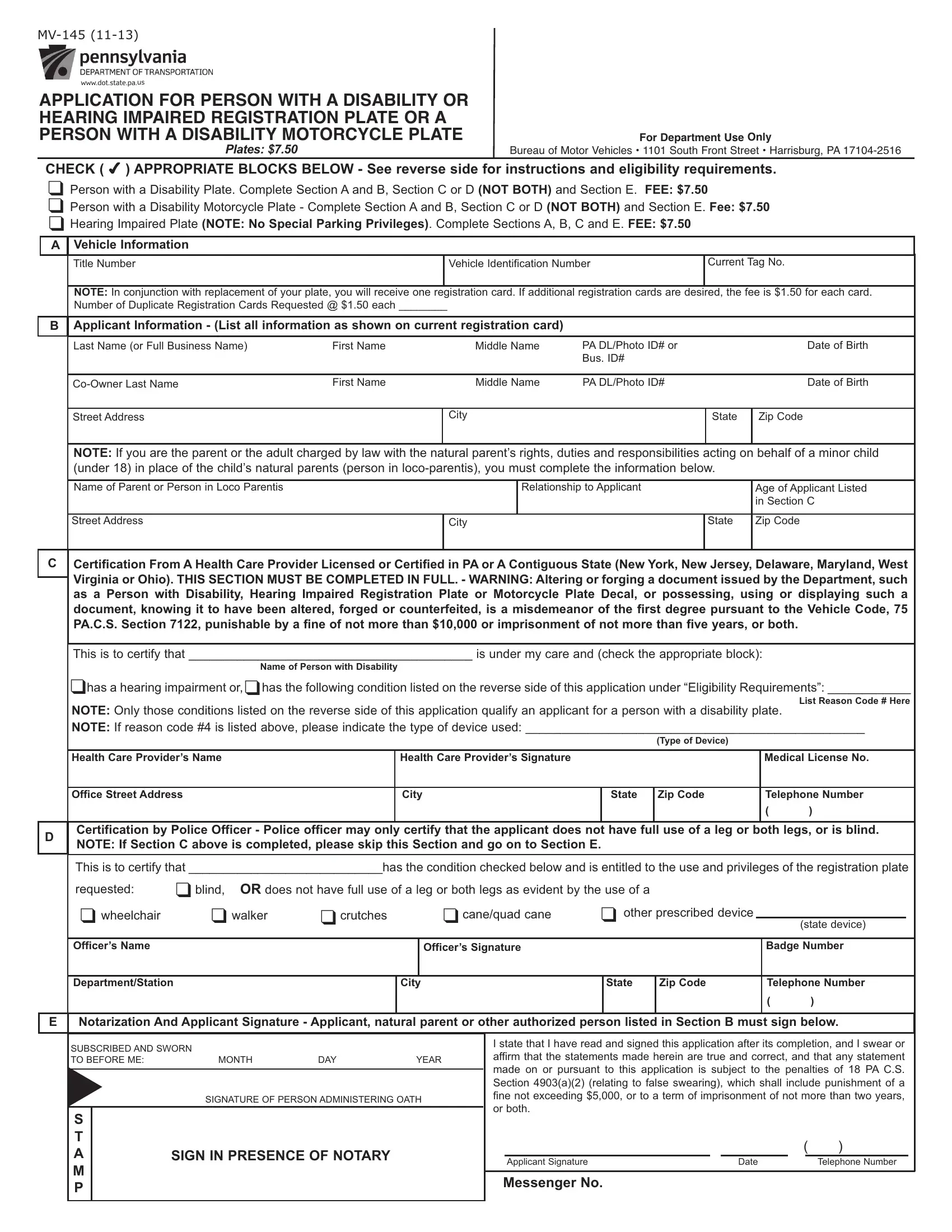
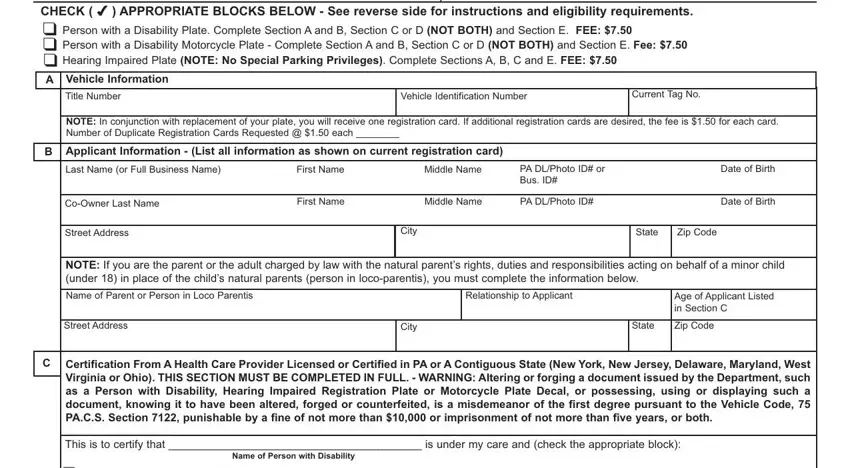
1. To begin with, while filling in the pa form 145, start with the area containing following fields:
2. Once your current task is complete, take the next step – fill out all of these fields - has a hearing impairment or has, NOTE Only those conditions listed, Health Care Providers Name, Health Care Providers Signature, Medical License No, Type of Device, Office Street Address, City, State, Zip Code, Telephone Number, Certification by Police Officer, This is to certify that has the, requested, and blind OR does not have full use of with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
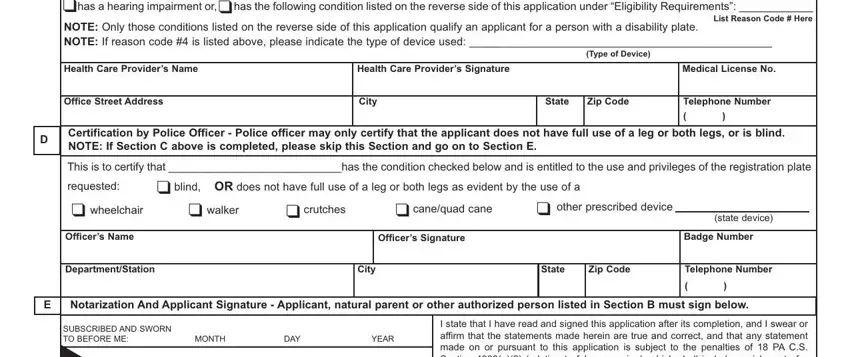
Always be very attentive while filling in blind OR does not have full use of and Health Care Providers Signature, since this is the section where most users make errors.
3. In this specific stage, take a look at SIGNATURE OF PERSON ADMINISTERING, S T A M P, I state that I have read and, SIGN IN PRESENCE OF NOTARY, Applicant Signature, Messenger No, Date, and Telephone Number. All these will need to be filled in with utmost precision.

Step 3: Be certain that your information is correct and then just click "Done" to conclude the task. Sign up with FormsPal right now and immediately obtain pa form 145, prepared for downloading. Each change you make is conveniently preserved , which enables you to modify the pdf later anytime. FormsPal ensures your information confidentiality by using a protected method that never records or shares any sort of private information used in the PDF. Be confident knowing your paperwork are kept safe each time you use our editor!