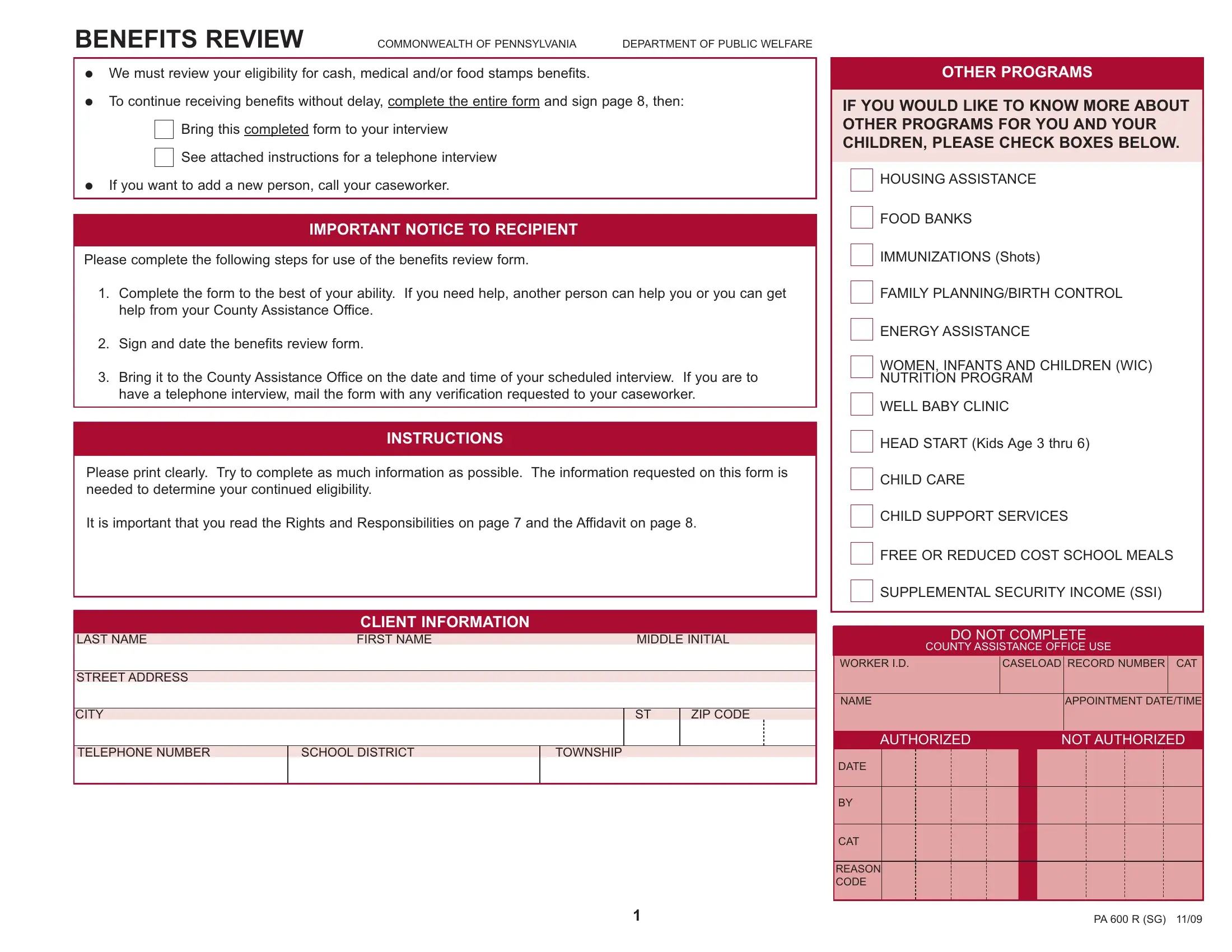
In the heart of Pennsylvania, the PA600R form serves as a crucial tool for individuals receiving benefits under the Commonwealth's Department of Public Welfare. This comprehensive document is designed to review eligibility for cash, medical, and food stamps benefits, ensuring that assistance continues without delay for those in need. The form demands careful completion and a signature on page 8, offering individuals the option to facilitate their review through an in-person or telephone interview. Its detailed sections call for information regarding client demographics, household composition, income, resources, and changes since the last review, emphasizing the necessity of transparency and accuracy. Additionally, the PA600R integrates matters of voter registration and health insurance, highlighting Pennsylvania's commitment to holistic welfare. The process outlined by the form not only aids in the efficient management of benefits but also underscores important legal notices and steps to ensure that applicants' rights are protected throughout the review process. By encapsulating a wide array of information pertinent to an individual’s eligibility and fostering an understanding of related programs and assistance, the PA600R form plays a pivotal role in the sustenance of Pennsylvania’s safety net for its residents.
| Question | Answer |
|---|---|
| Form Name | Pa600R Form |
| Form Length | 10 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 30 sec |
| Other names | pennsylvania 600r, pa 600 r benefits review, pa600r form pdf, pa r sg public welfare |
