


application paad can be filled out online without any problem. Just open FormsPal PDF tool to perform the job fast. We at FormsPal are aimed at providing you the absolute best experience with our tool by constantly introducing new capabilities and upgrades. With these improvements, using our tool gets easier than ever before! It merely requires a couple of basic steps:
Step 1: Simply hit the "Get Form Button" in the top section of this page to start up our form editor. This way, you'll find everything that is necessary to fill out your document.
Step 2: The tool will allow you to change PDF files in a range of ways. Transform it by writing your own text, correct what is already in the file, and place in a signature - all readily available!
This PDF form will need specific information; to guarantee accuracy, please be sure to consider the next recommendations:
1. You will want to fill out the application paad accurately, so be mindful while filling out the sections containing these particular blank fields:
2. After the last array of fields is complete, it's time to put in the needed details in Disabled Program, wwwnjpaadgov, PAAD beneficiaries must fill out, Income limit less than single, ID Number starts with, PAAD copay is, per PAAD covered generic drug, Catastrophic cap does not apply, Senior Gold Prescription Discount, wwwnjsrgoldgov, single married, and Senior Gold beneficiaries do not so you can go further.
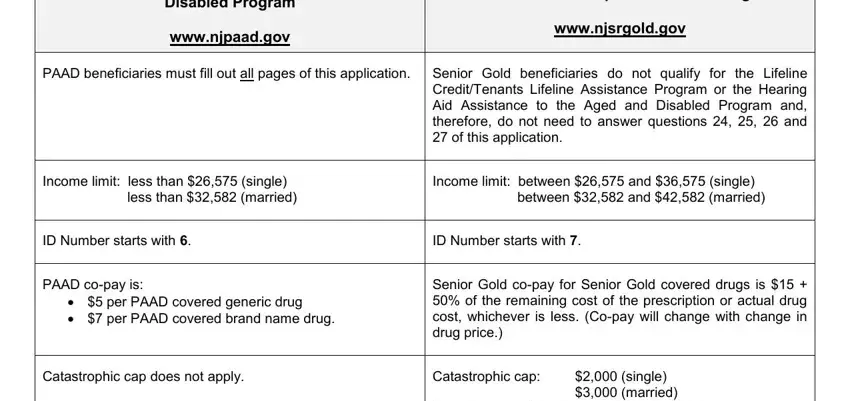
Concerning Income limit less than single and PAAD beneficiaries must fill out, make certain you double-check them in this section. Both of these could be the key fields in the document.
Step 3: Glance through the information you've typed into the form fields and click on the "Done" button. After creating a7-day free trial account here, it will be possible to download application paad or send it via email directly. The PDF document will also be accessible via your personal account page with your every single change. FormsPal is invested in the privacy of all our users; we make certain that all personal information processed by our tool stays secure.