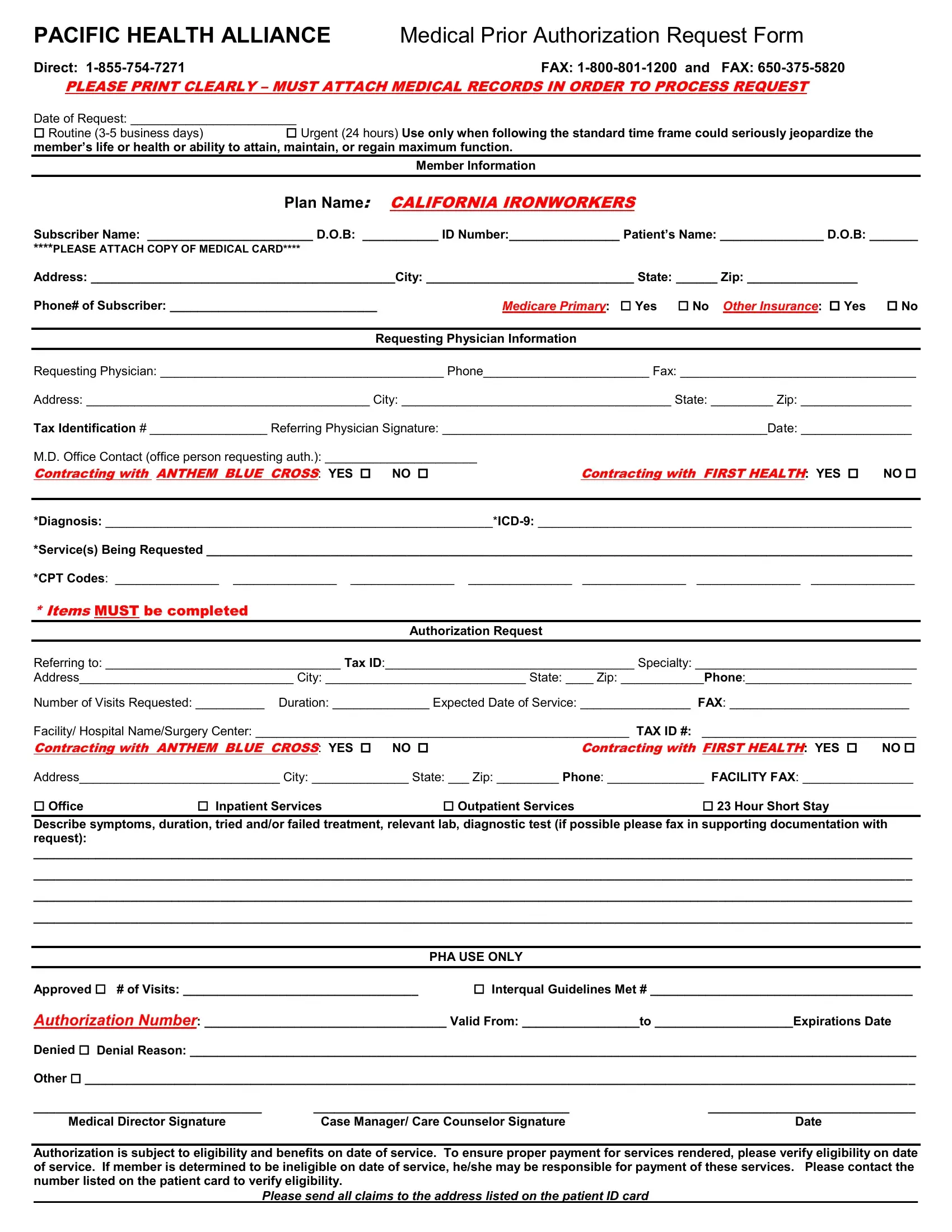
The Pacific Health Alliance Medical Prior Authorization Request Form embodies a critical process in healthcare management, serving as a gateway for securing necessary medical services. This detailed form, designed for streamlined communication between healthcare providers and the insurance company, necessitates comprehensive information to ensure a smooth authorization process. It outlines specific sections for both routine and urgent requests, clearly marking the urgency of medical intervention required and emphasizing the need for attached medical records to process the request efficiently. From capturing essential member and physician details, such as names, contact information, and insurance specifics, to listing the requested medical services with appropriate diagnostic codes, every section is tailored to gather requisite data. Moreover, the form goes beyond mere data collection by instructing providers on how to classify the requested services—ranging from office visits to inpatient or outpatient services—and demanding a detailed account of the patient's symptoms, treatment history, and diagnostic tests. The addition of sections indicating whether the provider is contracting with significant insurers like Anthem Blue Cross and First Health highlights the form's role in navigating the complex insurance landscape. Ultimately, this document culminates in a section for Pacific Health Alliance's use only, delineating the approval or denial of the request, thus governing the patient's access to the proposed healthcare services based on criteria like eligibility and benefit coverage on the service date, underscoring the importance of verification to avoid unexpected patient liabilities.
| Question | Answer |
|---|---|
| Form Name | Pacific Alliance Medical Group Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | community care alliance prior auth form for surger, pacific health alliance prior authorization, health alliance prior auth forms, central california alliance prior authorization form dme fillable |
PACIFIC HEALTH ALLIANCE Medical Prior Authorization Request Form
Direct: |
FAX: |
PLEASE PRINT CLEARLY – MUST ATTACH MEDICAL RECORDS IN ORDER TO PROCESS REQUEST |
|
Date of Request: ________________________ |
|
Routine |
Urgent (24 hours) Use only when following the standard time frame could seriously jeopardize the |
member’s life or health or ability to attain, maintain, or regain maximum function.
Member Information
Plan Name: CALIFORNIA IRONWORKERS
Subscriber Name: ________________________ D.O.B: ___________ ID Number:________________ Patient’s Name: _______________ D.O.B: _______
****PLEASE ATTACH COPY OF MEDICAL CARD****
Address: ____________________________________________City: ______________________________ State: ______ Zip: ________________
Phone# of Subscriber: ______________________________Medicare Primary: Yes No Other Insurance: Yes No
Requesting Physician Information
Requesting Physician: _________________________________________ Phone________________________ Fax: __________________________________
Address: _________________________________________ City: _______________________________________ State: _________ Zip: ________________
Tax Identification # _________________ Referring Physician Signature: _______________________________________________Date: ________________
M.D. Office Contact (office person requesting auth.): ______________________
Contracting with ANTHEM BLUE CROSS: YES NO Contracting with FIRST HEALTH: YES NO
*Diagnosis:
*Service(s) Being Requested ______________________________________________________________________________________________________
*CPT Codes: _______________ _______________ _______________ _______________ _______________ _______________ _______________
*Items MUST be completed
Authorization Request
Referring to: __________________________________ Tax ID:____________________________________ Specialty: ________________________________
Address_______________________________ City: _____________________________ State: ____ Zip: ____________Phone:________________________
Number of Visits Requested: __________ Duration: ______________ Expected Date of Service: ________________ FAX: __________________________
Facility/ Hospital Name/Surgery Center: ______________________________________________________ TAX ID #: _______________________________
Contracting with ANTHEM BLUE CROSS: YES NO Contracting with FIRST HEALTH: YES NO
Address_____________________________ City: ______________ State: ___ Zip: _________ Phone: ______________ FACILITY FAX: ________________
Office Inpatient Services Outpatient Services 23 Hour Short Stay
Describe symptoms, duration, tried and/or failed treatment, relevant lab, diagnostic test (if possible please fax in supporting documentation with request):
_______________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________
PHA USE ONLY
Approved # of Visits: __________________________________ Interqual Guidelines Met # ______________________________________
Authorization Number: ___________________________________ Valid From: _________________to ____________________Expirations Date
Denied Denial Reason: _________________________________________________________________________________________________________
Other ________________________________________________________________________________________________________________________
_________________________________ |
_____________________________________ |
______________________________ |
Medical Director Signature |
Case Manager/ Care Counselor Signature |
Date |
Authorization is subject to eligibility and benefits on date of service. To ensure proper payment for services rendered, please verify eligibility on date of service. If member is determined to be ineligible on date of service, he/she may be responsible for payment of these services. Please contact the number listed on the patient card to verify eligibility.
Please send all claims to the address listed on the patient ID card_______________________________________