Have you ever visited a doctor or specialist and been asked to fill out a past medical history form? It can be an intimidating task, with questions that cover the spectrum of your health concerns and conditions. While many of us would prefer to avoid this step in the healthcare process, it is important for understanding your current state of wellness. Gathering information from your past medical history helps ensure that doctors have as complete a picture as possible when making diagnosis and treatment decisions - ultimately providings you with better care. In this post, we'll walk through why gathering this type of data is so important, what types of questions are typically asked, when these forms should be filled out, and more!
| Question | Answer |
|---|---|
| Form Name | Past Medical History Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | physical past medical form, physician history forms, therapy past medical sample, physical therapy past medical form |
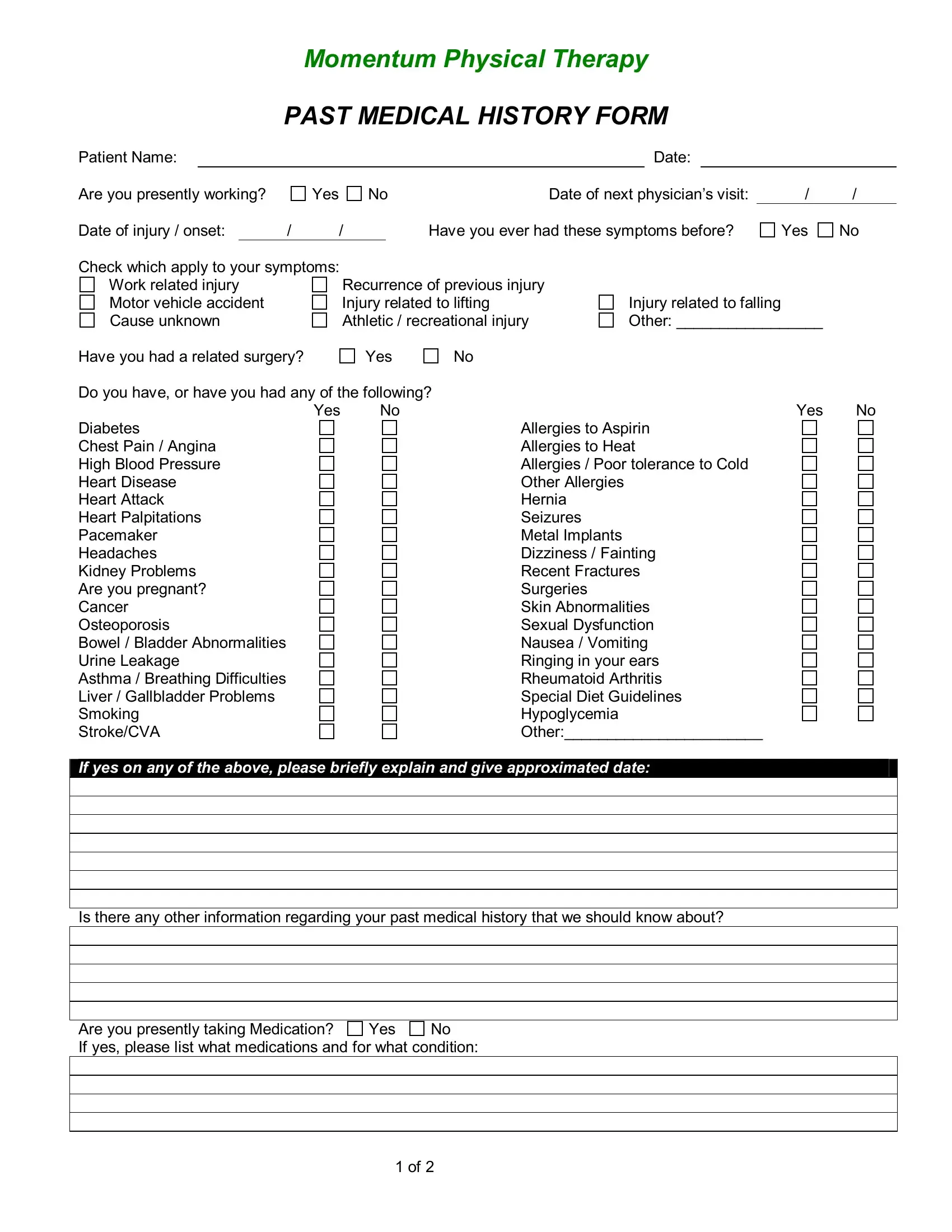
Momentum Physical Therapy
PAST MEDICAL HISTORY FORM
Patient Name:
Are you presently working?
Date of injury / onset: |
/ |
Yes
/
Date:
No |
Date of next physician’s visit: |
Have you ever had these symptoms before?
/ /
Yes No
Check which apply to your symptoms: |
|
|
Work related injury |
Recurrence of previous injury |
|
Motor vehicle accident |
Injury related to lifting |
|
Cause unknown |
Athletic / recreational injury |
|
Have you had a related surgery? |
Yes |
No |
Injury related to falling Other: _________________
Do you have, or have you had any of the following? |
|
|
|
Yes |
No |
Yes |
No |
Diabetes |
|
Allergies to Aspirin |
|
Chest Pain / Angina |
|
Allergies to Heat |
|
High Blood Pressure |
|
Allergies / Poor tolerance to Cold |
|
Heart Disease |
|
Other Allergies |
|
Heart Attack |
|
Hernia |
|
Heart Palpitations |
|
Seizures |
|
Pacemaker |
|
Metal Implants |
|
Headaches |
|
Dizziness / Fainting |
|
Kidney Problems |
|
Recent Fractures |
|
Are you pregnant? |
|
Surgeries |
|
Cancer |
|
Skin Abnormalities |
|
Osteoporosis |
|
Sexual Dysfunction |
|
Bowel / Bladder Abnormalities |
|
Nausea / Vomiting |
|
Urine Leakage |
|
Ringing in your ears |
|
Asthma / Breathing Difficulties |
|
Rheumatoid Arthritis |
|
Liver / Gallbladder Problems |
|
Special Diet Guidelines |
|
Smoking |
|
Hypoglycemia |
|
Stroke/CVA |
|
Other:_______________________ |
|
If yes on any of the above, please briefly explain and give approximated date:
Is there any other information regarding your past medical history that we should know about?
Are you presently taking Medication? |
Yes |
No |
If yes, please list what medications and for what condition:
1 of 2
In the rare instance of an emergency, whom should we contact?
Name:
Phone Number:
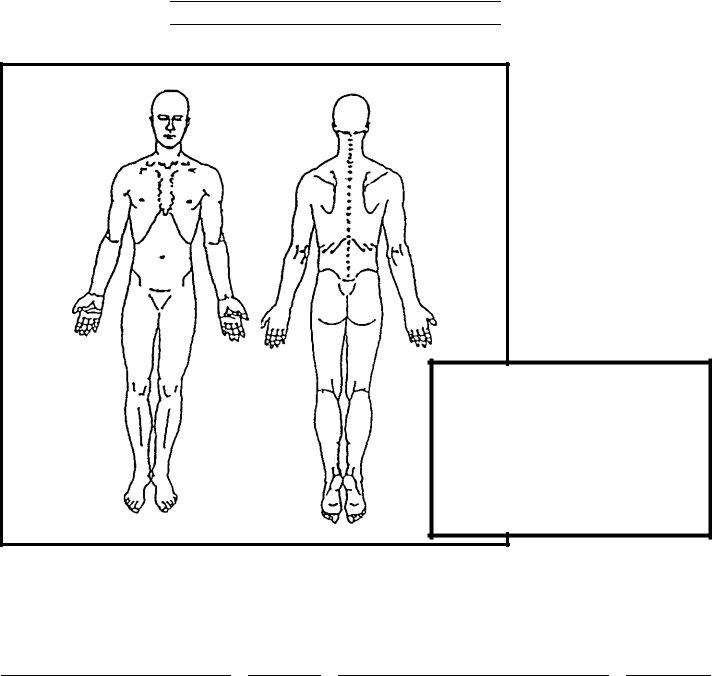
Please indicate below where your symptoms are located.
KEY: |
|
Numbness |
======== |
Pins & Needles |
ooooooo |
Burning Pain |
xxxxxxxx |
Stabbing Pain |
/ / / / / / / / |
|
|
If you are having pain, please rate the intensity of your pain on a scale of 0 to 10, with 0 being no pain and 10 being the worst pain possible: ___________________.
Patient’s Signature |
Date |
Signature of Guardian if patient is a minor |
Date |
||
|
/ |
/ |
|
|
|
Therapist Signature |
|
Date |
|
|
|
2 of 2