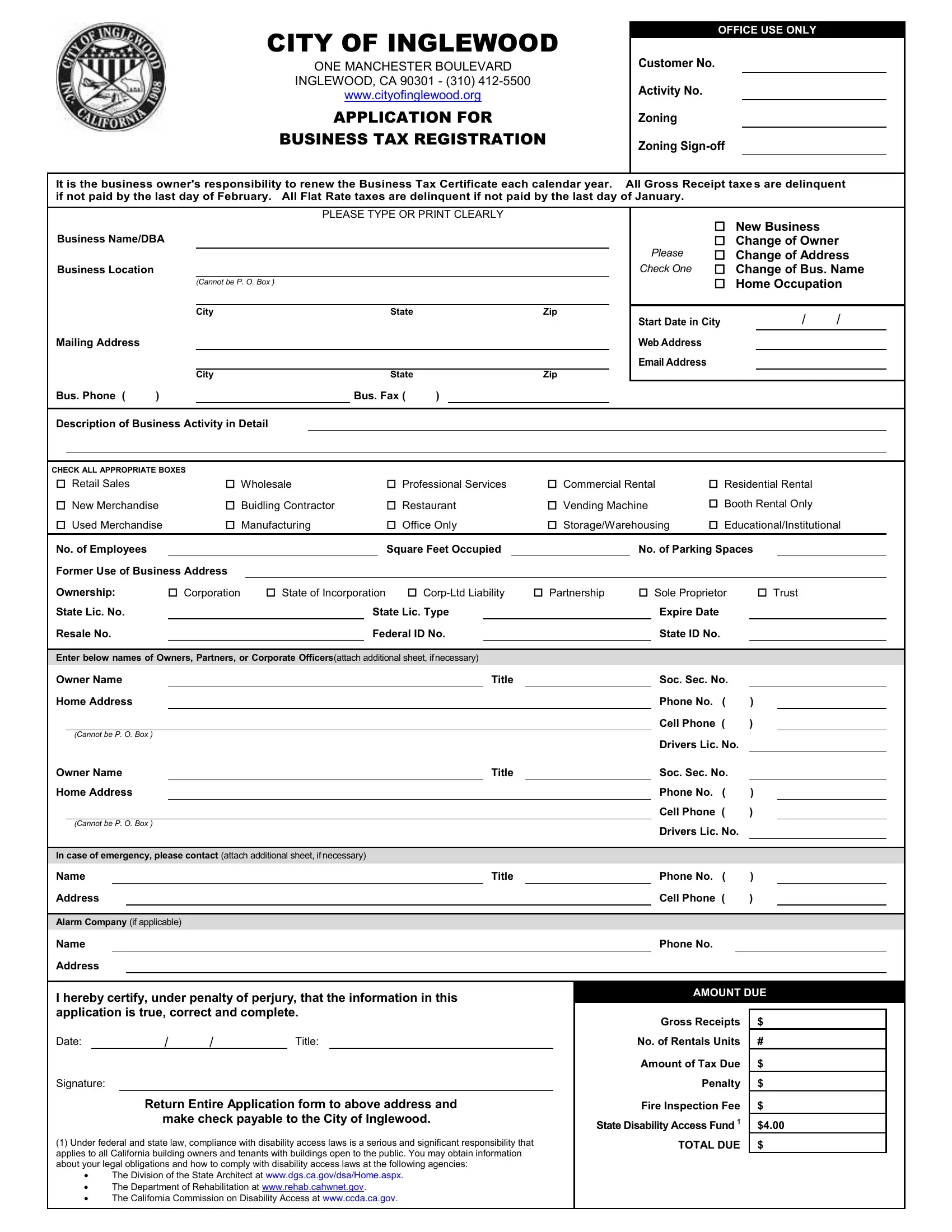
In the bustling city of Inglewood, California, the dynamics of operating a business include the pivotal step of obtaining a Business Tax Certificate, a process meticulously outlined in their official "Application for Business Tax Registration." This document is not just a formality but a comprehensive gateway that ensures businesses are properly registered and aligned with the city's regulatory requirements. It encompasses a broad spectrum of details, from basic information such as the business name, location, and contact details, to more specific aspects like the nature of the business activity, zoning compliance, and emergency contacts. The form also prompts applicants to indicate their business structure—be it a corporation, partnership, or sole proprietorship—alongside requisite state and federal identification numbers. Special attention is given to the fiscal responsibilities associated with the certificate, including deadlines for tax payments based on gross receipts or flat rates, thereby underlining the importance of timely compliance. Moreover, the inclusion of accessibility compliance information highlights the city's commitment to ensuring that businesses are accessible to all, reflecting broader federal and state legal obligations. Through the lens of this form, the City of Inglewood not only facilitates business operations but also fosters a regulated, inclusive, and thriving business environment.
| Question | Answer |
|---|---|
| Form Name | Pay Business Tax Certificate Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Business Tax Certificate Application - City of Inglewood |
CITY OF INGLEWOOD
ONE MANCHESTER BOULEVARD
INGLEWOOD, CA 90301 - (310)
www.cityofinglewood.org
APPLICATION FOR
BUSINESS TAX REGISTRATION
OFFICE USE ONLY
Customer No.
Activity No.
Zoning
Zoning
It is the business owner's responsibility to renew the Business Tax Certificate each calendar year. All Gross Receipt taxes are delinquent if not paid by the last day of February. All Flat Rate taxes are delinquent if not paid by the last day of January.
|
|
|
PLEASE TYPE OR PRINT CLEARLY |
|||
Business Name/DBA |
|
|
|
|
||
Business Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CANNOT BE P. O. BOX ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
|
Zip |
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
State |
|
Zip |
Bus. Phone ( |
) |
|
|
Bus. Fax ( |
) |
|
|
New Business |
|
Change of Owner |
PLEASE |
Change of Address |
CHECK ONE |
Change of Bus. Name |
|
Home Occupation |
Start Date in City |
/ |
/ |
Web Address |
|
|
Email Address |
|
|
Description of Business Activity in Detail
CHECK ALL APPROPRIATE BOXES |
|
|
|
|
Retail Sales |
Wholesale |
Professional Services |
Commercial Rental |
Residential Rental |
New Merchandise |
Buidling Contractor |
Restaurant |
Vending Machine |
Booth Rental Only |
Used Merchandise |
Manufacturing |
Office Only |
Storage/Warehousing |
Educational/Institutional |
|
No. of Employees |
|
|
|
|
|
|
|
Square Feet Occupied |
|
|
|
|
|
No. of Parking Spaces |
|
|
||||||||||
|
Former Use of Business Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Ownership: |
|
Corporation |
State of Incorporation |
|
Partnership |
Sole Proprietor |
Trust |
|
||||||||||||||||||
|
State Lic. No. |
|
|
|
|
|
|
State Lic. Type |
|
|
|
|
|
|
Expire Date |
|
|
|
|||||||||
|
Resale No. |
|
|
|
|
|
|
|
|
|
Federal ID No. |
|
|
|
|
|
|
State ID No. |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Enter below names of Owners, Partners, or Corporate Officers(attach additional sheet, ifnecessary) |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
Owner Name |
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
Soc. Sec. No. |
|
|
|
|||||||
|
Home Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. ( |
) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone ( |
) |
|
|
|
|
|
(CANNOT BE P. O. BOX ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drivers Lic. No. |
|
|
|
|
|
Owner Name |
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
Soc. Sec. No. |
|
|
|
|||||||
|
Home Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. ( |
) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone ( |
) |
|
|
|
|
|
(CANNOT BE P. O. BOX ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drivers Lic. No. |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
In case of emergency, please contact (attach additional sheet, ifnecessary) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
Phone No. ( |
) |
|
|
||||
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell Phone ( |
) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Alarm Company (if applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone No. |
|
|
|
|||
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
I hereby certify, under penalty of perjury, that the information in this |
|
|
|
|
|
AMOUNT DUE |
|
|||||||||||||||||||
|
application is true, correct and complete. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
Gross Receipts |
$ |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Date: |
|
|
|
/ |
/ |
|
Title: |
|
|
|
|
|
|
|
No. of Rentals Units |
# |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount of Tax Due |
$ |
|
|
||
|
Signature: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Penalty |
$ |
|
|
|||
|
|
|
|
|
|
Return Entire Application form to above address and |
|
|
|
|
Fire Inspection Fee |
$ |
|
|
|||||||||||||
|
|
|
|
|
|
|
make check payable to the City of Inglewood. |
|
|
|
State Disability Access Fund 1 |
$4.00 |
|
||||||||||||||
|
(1) Under federal and state law, compliance with disability access laws is a serious and significant responsibility that |
|
|
|
TOTAL DUE |
$ |
|
|
|||||||||||||||||||
|
applies to all California building owners and tenants with buildings open to the public. You may obtain information |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
about your legal obligations and how to comply with disability access laws at the following agencies: |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
∙ |
The Division of the State Architect at www.dgs.ca.gov/dsa/Home.aspx. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
∙ |
The Department of Rehabilitation at www.rehab.cahwnet.gov. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
∙ |
The California Commission on Disability Access at www.ccda.ca.gov. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|